Downloaded 28 times






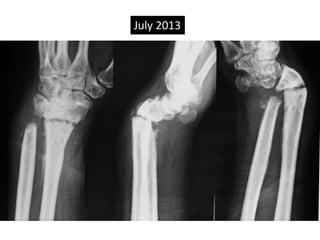

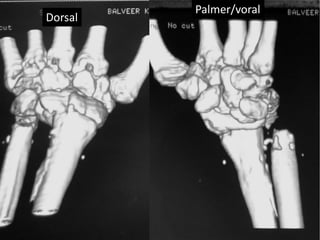
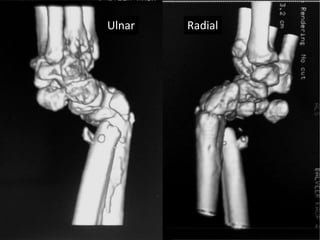


















This document reports on three cases of non-union of fractures of the lower end of the radius. Non-union of distal radius fractures is rare, with an incidence of around 0.2%. The cases presented had different clinical presentations and treatment histories, but all resulted in non-union of the radius. Early suspicion of potential non-union is important if x-rays at 6 weeks show a clear fracture line without signs of healing. Surgical treatment of non-union involves debridement, correction of any deformity, bone grafting and internal fixation. However, patient acceptance of corrective surgery can be poor given the minimal disability caused by the non-union in some cases.




















































![FOREARM_FRACTURES[1].pptx and management](https://cdn.slidesharecdn.com/ss_thumbnails/forearmfractures1-250813120934-75e3f6d7-thumbnail.jpg?width=640&height=640&fit=bounds)


![www corrected shahab '24 JC Colle's fracture [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/wwwcorrectedshahab24jccollesfractureautosaved-250519081914-6e733621-thumbnail.jpg?width=640&height=640&fit=bounds)









































