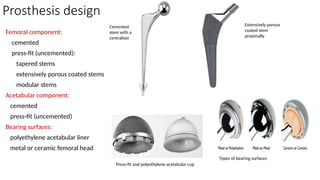
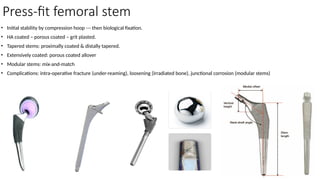
Prosthesis design
Femoral component:
cemented
press-fit(uncemented):
tapered stems
extensively porous coated stems
modular stems
Acetabular component:
cemented
press-fit (uncemented)
Bearing surfaces:
polyethylene acetabular liner
metal or ceramic femoral head
Cemented
stem with a
centralizer
Extensively porous
coated stem
proximally
Press-fit and polyethylene acetabular cup
Types of bearing surfaces
4.
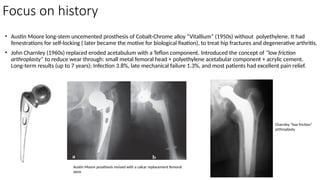
Focus on history
•Austin Moore long-stem uncemented prosthesis of Cobalt-Chrome alloy “Vitallium” (1950s) without polyethylene. It had
fenestrations for self-locking ( later became the motive for biological fixation), to treat hip fractures and degenerative arthritis.
• John Charnley (1960s) replaced eroded acetabulum with a Teflon component. Introduced the concept of “low friction
arthroplasty” to reduce wear through: small metal femoral head + polyethylene acetabular component + acrylic cement.
Long-term results (up to 7 years): Infection 3.8%, late mechanical failure 1.3%, and most patients had excellent pain relief.
Austin Moore prosthesis revised with a calcar replacement femoral
stem
Charnley “low friction”
arthroplasty
5.
Focus on history
Survivorshipof a Charnley total hip arthroplasty. A concise follow-up, at a minimum of thirty-five years, of previous reports.
• Callaghan JJ, Bracha P, Liu SS, Piyaworakhun S, Goetz DD, Johnston RC . J Bone Joint Surg Am. 2009 Nov;91(11):2617-21
• The purpose of this study was to update the results, at a minimum of thirty-five years, in a single-surgeon series of primary Charnley total hip arthroplasties performed with cement.
Twelve patients (fifteen hips) were alive, 249 patients (314 hips) had died, and one patient (one hip) had been lost to follow-up. Seven of the hips in the living patients had required at
least one revision; 290 (88%) of the original group of total hip prostheses either continued to function or were in patients who had died. Since the time of a thirty-year study of this
cohort, one hip that had previously been revised because of acetabular loosening required an additional revision because of acetabular loosening and two additional hips had evidence of
radiographic loosening (of one acetabular and one femoral component). The survival rate with revision for any reason as the end point was 78%. This end result study should provide a
benchmark for subsequent procedures and designs with the caveat that patient life expectancy will likely continue to increase and modern-design implants are being used in younger
patients.
Primary total hip arthroplasty with a flanged, cemented all-polyethylene acetabular component: evaluation at a minimum of 20 years.
• Della Valle CJ, Kaplan K, Jazrawi A, Ahmed S, Jaffe WL. J Arthroplasty. 2004 Jan;19(1):23-6
• One hundred twenty-three consecutive primary total hip arthroplasties in 107 patients were performed with the insertion of a cemented, all polyethylene, flanged acetabular
component. At a minimum of 20 years, 66 patients had died (75 hips) and 8 patients (8 hips) were lost to follow-up evaluation, leaving 40 hips in 33 patients. At a mean of 21.1 years, 2
cups had been revised for aseptic loosening, one well-fixed cup was revised at the time of femoral component revision, and 4 additional cups had definite evidence of radiographic
loosening. Survivorship analysis revealed a 77.3% survivorship for the component at 21 years, with revision or definite loosening as an endpoint (95% confidence interval, 67.8%-86.8%).
Charnley low-friction arthroplasty of the hip. Twenty-year results with cement.
• Kavanagh BF, Wallrichs S, Dewitz M, Berry D, Currier B, Ilstrup D, Coventry MB. J Arthroplasty. 1994 Jun;9(3):229-34.
• The first 333 Charnley (Thackray, United Kingdom) total hip arthroplasties performed at the Mayo Clinic between 1969 and 1970 have been followed since that time. One hundred twelve
patients (112 hips) remain alive at 20 years. Clinical results remain excellent. The Mayo clinical and roentgenographic hip scoring system rates the results as good to excellent in 39 of 69
hips (with all necessary data to calculate the entire score), fair in 13 hips, and poor in 17 hips. The clinical score alone showed satisfactory results in 77 of 112 hips. Some clinical
deterioration was attributed to the advancing age of the patients (mean age at final follow-up evaluation, 84 years). Probable roentgenographic loosening (component migration,
complete bone-cement interface, radiolucent line greater than 1 mm, cement fracture) was noted in 12 of 69 acetabular components (17%) and 28 of 69 femoral components (36%). Two
patients had required revision since the last report at 15 years for a total of 38 patients (32 revised, 4 Girdlestone arthroplasties, 2 stem fractures not yet revised). The probability of
surviving 20 years without revision of the components was 84% (83% for men, 85% for women). The rates of loosening, revision, and failure (revision, Girdlestone, or symptomatic
loosening) remain linear over 20 years of follow-up evaluation. If the probability of revision is based on patient age at the time of the initial total hip arthroplasty, there is a significantly
increased probability of revision in those patients less than 59 years of age (27%) compared to those 59-65 years of age (13%), 65-70 years (7.5%), and over 70 years (12%).
6.
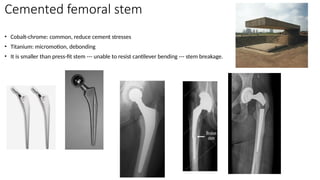
Cemented femoral stem
•Cobalt-chrome: common, reduce cement stresses
• Titanium: micromotion, debonding
• It is smaller than press-fit stem --- unable to resist cantilever bending --- stem breakage.
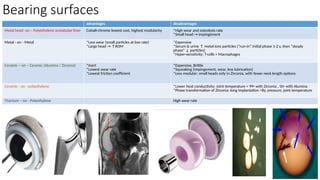
Bearing surfaces
advantages disadvantages
Metalhead- on – Polyethylene acetabular liner Cobalt-chrome lowest cost, highest modularity *High wear and osteolysis rate
*Small head → impingement
Metal - on - Metal *Less wear (small particles at low rate)
*Large head → ↑ROM
*Expensive
*Serum & urine ↑ metal ions particles (“run-in” initial phase 1-2 y, then “steady
phase” ↓ particles)
*Hyper-sensitivity: T-cells + Macrophages
Ceramic – on – Ceramic (Alumina / Zirconia) *Inert
*Lowest wear rate
*Lowest friction coefficient
*Expensive, Brittle
*Squeaking (impingement, wear, less lubrication)
*Less modular: small heads only in Zirconia, with fewer neck length options
Ceramic - on - polyethylene *Lower heat conductivity: Joint temperature = 99◦ with Zirconia , 50◦ with Alumina
*Phase transformation of Zirconia: long implantation >8y, pressure, joint temperature
Titanium – on - Polyethylene High wear rate
9.
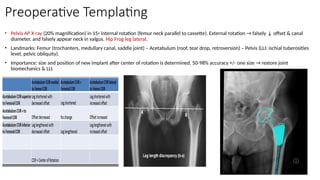
Preoperative Templating
• PelvisAP X-ray (20% magnification) in 15◦ internal rotation (femur neck parallel to cassette). External rotation → falsely ↓ offset & canal
diameter, and falsely appear neck in valgus. Hip Frog leg lateral.
• Landmarks: Femur (trochanters, medullary canal, saddle joint) – Acetabulum (roof, tear drop, retroversion) – Pelvis (LLI: ischial tuberosities
level, pelvic obliquity).
• Importance: size and position of new implant after center of rotation is determined. 50-98% accuracy +/- one size → restore joint
biomechanics & LLI.
10.
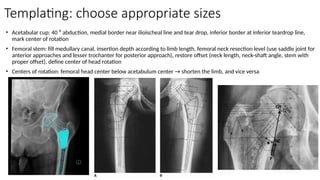
Templating: choose appropriatesizes
• Acetabular cup: 40 ⁰ abduction, medial border near ilioischeal line and tear drop, inferior border at inferior teardrop line,
mark center of rotation
• Femoral stem: fill medullary canal, insertion depth according to limb length, femoral neck resection level (use saddle joint for
anterior approaches and lesser trochanter for posterior approach), restore offset (neck length, neck-shaft angle, stem with
proper offset), define center of head rotation
• Centers of rotation: femoral head center below acetabulum center → shorten the limb, and vice versa
11.
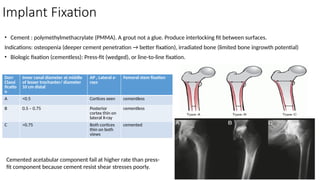
Implant Fixation
• Cement: polymethylmethacrylate (PMMA). A grout not a glue. Produce interlocking fit between surfaces.
Indications: osteopenia (deeper cement penetration → better fixation), irradiated bone (limited bone ingrowth potential)
• Biologic fixation (cementless): Press-fit (wedged), or line-to-line fixation.
Dorr
Classi
ficatio
n
Inner canal diameter at middle
of lesser trochanter/ diameter
10 cm distal
AP , Lateral x-
rays
Femoral stem fixation
A <0.5 Cortices seen cementless
B 0.5 – 0.75 Posterior
cortex thin on
lateral X-ray
cementless
C >0.75 Both cortices
thin on both
views
cemented
Cemented acetabular component fail at higher rate than press-
fit component because cement resist shear stresses poorly.
12.
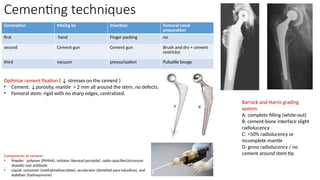
Cementing techniques
Generation Mixingby Insertion Femoral canal
preparation
first hand Finger packing no
second Cement gun Cement gun Brush and dry + cement
restrictor
third vacuum pressurization Pulsatile lavage
Optimize cement fixation ( ↓ stresses on the cement )
• Cement: ↓porosity, mantle > 2 mm all around the stem, no defects.
• Femoral stem: rigid with no sharp edges, centralized.
Barrack and Harris grading
system
A: complete filling (white-out)
B: cement-bone interface slight
radiolucency
C: >50% radiolucency or
incomplete mantle
D: gross radiolucency / no
cement around stem tip
Components of cement:
• Powder : polymer (PMMA), initiator (benzoyl peroxide), radio-opacifier(zirconium
dioxide) and antibiotic
• Liquid: monomer (methylmethacrylate), accelerator (dimethyl para-toluidine), and
stabilizer (hydroquinone)
13.
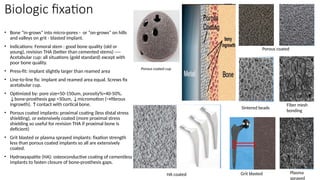
Biologic fixation
• Bone“in-grows” into micro-pores - or “on-grows” on hills
and valleys on grit - blasted implant.
• Indications: Femoral stem : good bone quality (old or
young), revision THA (better than cemented stems) ----
Acetabular cup: all situations (gold standard) except with
poor bone quality.
• Press-fit: implant slightly larger than reamed area
• Line-to-line fix: implant and reamed area equal. Screws fix
acetabular cup.
• Optimized by: pore size=50-150um, porosity%=40-50%,
↓bone-prosthesis gap <50um, ↓micromotion (→fibrous
ingrowth), ↑contact with cortical bone.
• Porous coated implants: proximal coating (less distal stress
shielding), or extensively coated (more proximal stress
shielding so useful for revision THA if proximal bone is
deficient)
• Grit blasted or plasma sprayed implants: fixation strength
less than porous coated implants so all are extensively
coated.
• Hydroxyapatite (HA): osteoconductive coating of cementless
implants to fasten closure of bone-prosthesis gaps.
Porous coated
Sintered beads
Fiber mesh
bonding
Grit blasted Plasma
sprayed
Porous coated cup
HA coated
14.
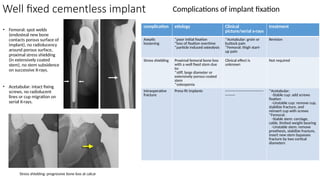
Well fixed cementlessimplant
• Femoral: spot welds
(endosteal new bone
contacts porous surface of
implant), no radiolucency
around porous surface,
proximal stress shielding
(in extensively coated
stem), no stem subsidence
on successive X-rays.
• Acetabular: intact fixing
screws, no radiolucent
lines or cup migration on
serial X-rays.
complication etiology Clinical
picture/serial x-rays
treatment
Aseptic
loosening
*poor initial fixation
*loss of fixation overtime
*particle induced osteolysis
*Acetabular: groin or
buttock pain
*Femoral: thigh start-
up pain
Revision
Stress shielding Proximal femoral bone loss
with a well fixed stem due
to:
*stiff, large diameter or
extensively porous coated
stem
*osteopenia
Clinical effect is
unknown
Not required
Intraoperative
fracture
Press-fit implants -------------------------------
--------
*Acetabular:
-Stable cup: add screws
fixation
-Unstable cup: remove cup,
stabilize fracture, and
reinsert cup with screws
*Femoral:
-Stable stem: cerclage,
cable, limited weight bearing
-Unstable stem: remove
prosthesis, stabilize fracture,
insert new stem bypasses
fracture by two cortical
diameters
Complications of implant fixation
Stress shielding: progressive bone loss at calcar
15.
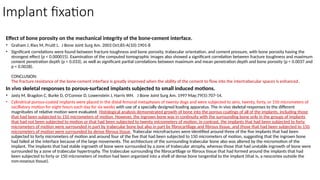
Implant fixation
Effect ofbone porosity on the mechanical integrity of the bone-cement interface.
• Graham J, Ries M, Pruitt L. J Bone Joint Surg Am. 2003 Oct;85-A(10):1901-8
• Significant correlations were found between fracture toughness and bone porosity, trabecular orientation, and cement pressure, with bone porosity having the
strongest effect (p < 0.000015). Examination of the computed tomographic images also showed a significant correlation between fracture toughness and maximum
cement penetration depth (p < 0.033), as well as significant partial correlations between maximum and mean penetration depth and bone porosity (p < 0.0037 and
p < 0.0028).
CONCLUSION:
The fracture resistance of the bone-cement interface is greatly improved when the ability of the cement to flow into the intertrabecular spaces is enhanced.
In vivo skeletal responses to porous-surfaced implants subjected to small induced motions.
• Jasty M, Bragdon C, Burke D, O'Connor D, Lowenstein J, Harris WH. J Bone Joint Surg Am. 1997 May;79(5):707-14.
• Cylindrical porous-coated implants were placed in the distal femoral metaphyses of twenty dogs and were subjected to zero, twenty, forty, or 150 micrometers of
oscillatory motion for eight hours each day for six weeks with use of a specially designed loading apparatus. The in vivo skeletal responses to the different
magnitudes of relative motion were evaluated. Histological analysis demonstrated growth of bone into the porous coatings of all of the implants, including those
that had been subjected to 150 micrometers of motion. However, the ingrown bone was in continuity with the surrounding bone only in the groups of implants
that had not been subjected to motion or that had been subjected to twenty micrometers of motion; in contrast, the implants that had been subjected to forty
micrometers of motion were surrounded in part by trabecular bone but also in part by fibrocartilage and fibrous tissue, and those that had been subjected to 150
micrometers of motion were surrounded by dense fibrous tissue. Trabecular microfractures were identified around three of the five implants that had been
subjected to forty micrometers of motion and around four of the five that had been subjected to 150 micrometers of motion, suggesting that the ingrown bone
had failed at the interface because of the large movements. The architecture of the surrounding trabecular bone also was altered by the micromotion of the
implant. The implants that had stable ingrowth of bone were surrounded by a zone of trabecular atrophy, whereas those that had unstable ingrowth of bone were
surrounded by a zone of trabecular hypertrophy. The trabeculae surrounding the fibrocartilage or fibrous tissue that had formed around the implants that had
been subjected to forty or 150 micrometers of motion had been organized into a shell of dense bone tangential to the implant (that is, a neocortex outside the
non-osseous tissue).
16.
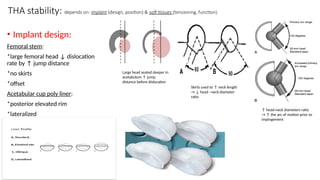
THA stability: dependson: implant (design, position) & soft tissues (tensioning, function).
• Implant design:
Femoral stem:
*large femoral head ↓ dislocation
rate by ↑ jump distance
*no skirts
*offset
Acetabular cup poly liner:
*posterior elevated rim
*lateralized
↑ head-neck diameters ratio
→ ↑ the arc of motion prior to
impingement
Skirts used to ↑ neck length
→ ↓ head –neck diameter
ratio
Large head seated deeper in
acetabulum ↑ jump
distance before dislocation
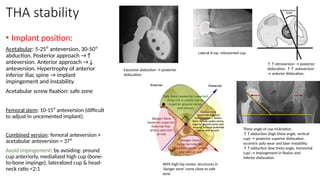
17.
THA stability
• Implantposition:
Acetabular: 5-25⁰ anteversion, 30-50⁰
abduction. Posterior approach →↑
anteversion. Anterior approach →↓
anteversion. Hypertrophy of anterior
inferior iliac spine → implant
impingement and instability.
Acetabular screw fixation: safe zone
Femoral stem: 10-15⁰ anteversion (difficult
to adjust in uncemented implant).
Combined version: femoral anteversion +
acetabular anteversion = 37⁰
Avoid impingement: by avoiding: pround
cup anteriorly, medialized high cup (bone-
to-bone impinge), lateralized cup & head-
neck ratio <2:1
↑↑retroversion → posterior
dislocation. ↑↑ anteversion
→ anterior dislocation.
Theta angle of cup inclination.
↑↑abduction (high theta angle, vertical
cup) → posterior superior dislocation ,
eccentric poly wear and later instability.
↑↑adduction (low theta angle, horizontal
cup) → impingement in flexion and
inferior dislocation.
Lateral X-ray: retroverted cup
Excessive abduction → posterior
dislocation
With high hip center, structures in
‘danger zone’ come close to safe
zone
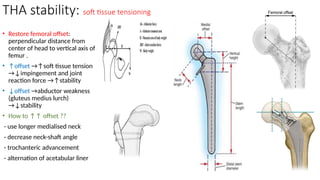
18.
THA stability: softtissue tensioning
• Restore femoral offset:
perpendicular distance from
center of head to vertical axis of
femur .
• ↑offset →↑soft tissue tension
→↓impingement and joint
reaction force →↑stability
• ↓offset →abductor weakness
(gluteus medius lurch)
→↓stability
• How to ↑↑ offset ??
- use longer medialised neck
- decrease neck-shaft angle
- trochanteric advancement
- alternation of acetabular liner
19.
THA stability: softtissue function
• Factors affect proper
soft tissue function:
(1) Local soft tissue integrity:
trauma, weak muscles
(poor health, aging,
myopathy, collagen
disorders, irradiation),
malignancy and infection.
(2) Neuromuscular function:
CNS disorder (stroke,
dementia, myopathy,
Parkinsonism, MS,
alcoholism) or peripheral
nervous system disorder
(peripheral neuropathy,
paralysis/paresis, spinal
canal stenosis,
radiculopathy).
inferior
gluteal n
(L5, S1,2)
Superior
gluteal n
Superior gluteal nerve (L4,5, S1)
supplies gluteus medius and
minimus.
With standing on one leg these
muscles contract to keep the
pelvis leveled (a). With paralysis
of SGN or weakness of
abductors the pelvis will drop on
the contralateral side (b).
Abductors superficial group:
gluteal muscles & TFL
Abductors deep group
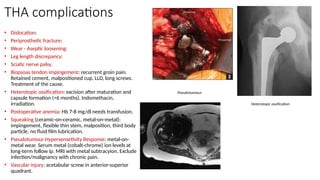
20.
THA complications
• Dislocation:
•Periprosthetic fracture:
• Wear - Aseptic loosening:
• Leg length discrepancy:
• Sciatic nerve palsy.
• Iliopsoas tendon impingement: recurrent groin pain.
Retained cement, malpositioned cup, LLD, long screws.
Treatment of the cause.
• Heterotopic ossification: excision after maturation and
capsule formation (>6 months). Indomethacin,
irradiation.
• Postoperative anemia: Hb 7-8 mg/dl needs transfusion.
• Squeaking (ceramic-on-ceramic, metal-on-metal):
impingement, flexible thin stem, malposition, third body
particle, no fluid film lubrication.
• Pseudotumour Hypersensetivity Response: metal-on-
metal wear. Serum metal (cobalt-chrome) ion levels at
long-term follow ip. MRI with metal subtracyion. Exclude
infection/malignancy with chronic pain.
• Vascular injury: acetabular screw in anterior-superior
quadrant.
Pseudotumour
Heterotopic ossification
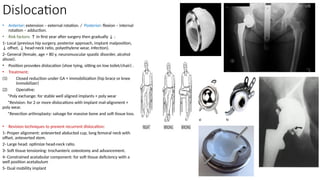
21.
Dislocation
• Anterior: extension– external rotation. / Posterior: flexion – internal
rotation – adduction.
• Risk factors: ↑ in first year after surgery then gradually ↓ :
1- Local (previous hip surgery, posterior approach, implant malposition,
↓ offset, ↓ head-neck ratio, polyethylene wear, infection).
2- General (female, age > 80 y, neuromuscular spastic disorder, alcohol
abuse).
• Position provokes dislocation (shoe tying, sitting on low toilet/chair) .
• Treatment:
(1) Closed reduction under GA + immobilization (hip brace or knee
immobilizer)
(2) Operative:
*Poly exchange: for stable well aligned implants + poly wear
*Revision: for 2 or more dislocations with implant mal-alignment +
poly wear.
*Resection arthroplasty: salvage for massive bone and soft tissue loss.
• Revision techniques to prevent recurrent dislocation:
1- Proper alignment: anteverted abducted cup, long femoral neck with
offset, anteverted stem.
2- Large head: optimize head-neck ratio.
3- Soft tissue tensioning: trochanteric osteotomy and advancement.
4- Constrained acetabular component: for soft tissue deficiency with a
well position acetabulum
5- Dual mobility implant
22.
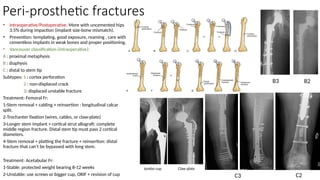
Peri-prosthetic fractures
• Intraoperative/Postoperative.More with uncemented hips
3.5% during impaction (implant size-bone mismatch).
• Prevention: templating, good exposure, reaming , care with
cementless implants in weak bones and proper positioning.
• Vancouver classification (intraoperative):
A : proximal metaphysis
B : diaphysis
C : distal to stem tip
Subtypes: 1 : cortex perforation
2 : non-displaced crack
3: displaced unstable fracture
Treatment: Femoral Fr:
1-Stem removal + cabling + reinsertion : longitudinal calcar
split.
2-Trochanter fixation (wires, cables, or claw-plate)
3-Longer stem implant + cortical strut allograft: complete
middle region fracture. Distal stem tip must pass 2 cortical
diameters.
4-Stem removal + platting the fracture + reinsertion: distal
fracture that can’t be bypassed with long stem.
Treatment: Acetabular Fr:
1-Stable: protected weight bearing 8-12 weeks
2-Unstable: use screws or bigger cup, ORIF + revision of cup
B2
B3
C2
Claw plate
C3
Jumbo cup
23.
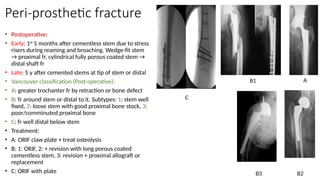
Peri-prosthetic fracture
• Postoperative:
•Early: 1st
5 months after cementless stem due to stress
risers during reaming and broaching. Wedge-fit stem
→ proximal fr, cylindrical fully porous coated stem →
distal shaft fr
• Late: 5 y after cemented stems at tip of stem or distal
• Vancouver classification (Post-operative):
• A: greater trochanter fr by retraction or bone defect
• B: fr around stem or distal to it. Subtypes: 1: stem well
fixed, 2: loose stem with good proximal bone stock, 3:
poor/comminuted proximal bone
• C: fr well distal below stem
• Treatment:
• A: ORIF claw plate + treat osteolysis
• B: 1: ORIF, 2: + revision with long porous coated
cementless stem, 3: revision + proximal allograft or
replacement
• C: ORIF with plate
A
B1
B2
B3
C
24.
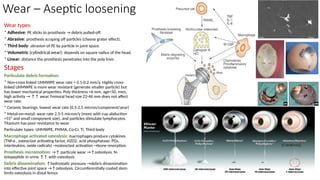
Wear – Asepticloosening
Wear types:
* Adhesive: PE sticks to prosthesis → debris pulled-off.
* Abrasive: prosthesis scraping off particles (cheese grater effect).
* Third body: abrasion of PE by particle in joint space.
* Volumetric (cylindrical wear): depends on square radius of the head.
* Linear: distance the prosthesis penetrates into the poly liner.
Stages
Particulate debris formation:
* Non-cross linked UHMWPE wear rate = 0.1-0.2 mm/y. Highly cross-
linked UHMWPE is more wear resistant (generate smaller particle) but
has lower mechanical properties. Poly thickness <6 mm, age<50, men,
high activity → ↑↑ wear. Femoral head size 22-46 mm does not affect
wear rate.
* Ceramic bearings: lowest wear rate (0.5-2.5 micron/component/year)
* Metal-on-metal: wear rate 2.5-5 micron/y (more with cup abduction
>55⁰ and small component size), and particles stimulate lymphocytes.
Titanium has poor resistance to wear.
Particulate types: UHMWPE, PMMA, Co-Cr, Ti, Third body
Macrophage activated osteolysis: macrophages produce cytokines
(TNf-α , osteoclast activating factor, H2O2, acid phosphatase, PGs,
interleukins, oxide radicals) →osteoclast activation →bone resorption.
Prosthesis micromotion: →↑ particule wear →↑osteolysis. N-
telopeptide in urine ↑↑ with osteolysis
Debris dissemination: ↑hydrostatic pressure →debris dissemination
into effective joint space →↑osteolysis. Circumferentially coated stem
limits osteolysis in distal femur.
25.
Osteolysis- Instability
Osteolysis inassociation with a total hip arthroplasty with ceramic bearing surfaces.
• Yoon TR, Rowe SM, Jung ST, Seon KJ, Maloney WJ. J Bone Joint Surg Am. 1998 Oct;80(10):1459-68
• The results of 103 total hip arthroplasties performed with insertion of a ceramic femoral head and acetabular component in ninety-six patients were
reviewed to determine the radiographic prevalence of osteolysis. After a mean duration of follow-up of ninety-two months (range, sixty to 125 months),
femoral osteolysis was observed in twenty-three hips (22 per cent), in one of two distinct patterns: linear osteolysis (twelve hips) or scalloping expansile-
type osteolysis (eleven hips). The most common locations of osteolysis in the femur were in zones I and VII as described by Gruen et al. Serial radiographs
demonstrated that the extent of the osteolysis progressed over time. Osteolysis of the pelvis, noted in forty-nine hips, was always associated with
migration of the acetabular socket. No focal osteolysis was observed in association with the stable sockets. Ten patients (ten hips) had a revision because
of loosening and migration of the acetabular component. In three of these patients, the femoral stem also was revised. Gross examination revealed
evidence of wear of the ceramic bearing surface in all ten patients. Scanning electron microscopy showed cracking and wear marks on the weight-bearing
surface. Histological evaluation of the tissue in the periprosthetic membrane demonstrated abundant ceramic wear particles. The interface membrane was
composed of a vascularized fibrous connective tissue with macrophages. Ultrastructurally, the macrophages contained numerous phagosomes of various
sizes, with electron-dense material within the cytoplasm of the cell. The mean size of the ceramic particles, as determined with scanning electron
microscopy, was 0.71 micrometer (range, 0.13 to 7.20 micrometers). This study supports the concept that ceramic wear particles can stimulate a foreign-
body response and periprosthetic osteolysis.
Instability after total hip arthroplasty: treatment with large femoral heads vs constrained liners.
• Sikes CV, Lai LP, Schreiber M, Mont MA, Jinnah RH, Seyler TM. J Arthroplasty. 2008 Oct;23(7 Suppl):59-63
• One of the most common complications after total hip arthroplasty is instability. This study reviewed the recent literature concerning the indications,
contraindications, and results of recent studies using both constrained liners and large femoral heads to treat instability after total hip arthroplasty. We
also report on the results of a series of 41 patients (52 hips) considered being at high risk for dislocation who were treated with large-diameter metal-on-
metal bearings and who were compared with a matched group of hips treated with standard-size metal-on-polyethylene bearings. The large-diameter
femoral head group had no dislocations at a minimum follow-up of 24 months, whereas the standard-size group had 2 dislocations. We support the use of
large femoral heads to treat instability in a wide variety of patients because of the increased stability, decreased wear of modern metal-on-metal designs,
increased range of motion, and variety of revision options.
26.
Aseptic loosening
• Pain(groin, thigh, or knee) ↑ with activity. Normal ESR, CRP.
• Serial X-rays: radiolucency > 1mm around implant or cement > 2 years
after surgery and stem subsidence. Focal ↑cortical density around
collar or tip of stem = non-uniform stress = loosening . Stem migration
(position relative to calcar). Cup migration: superior / medial > 2mm,
changes in version or inclination, screws breakage, or radiolucent line
> 1mm seen in the 3 zones.
• Treatment:
Observation (stable implant + minimal symptoms).
Operative: Revision + osteolysis grafting.
• Stem: Proxmially coated (primary implant): for sufficient metaphyseal
bone stock. Fully-coated (cylindrical monoblock): for deficient bone
stock. Fluted, Tapered (Wagner-type): monoblock/modular: for type
3B, and some type 4. Oncology prosthesis: for type 4 implants.
• Acetabular Cup:
• Osteolysis: Asymptomatic: implant revision/ retention + bone grafting
+ head/liner exchange; or close monitoring. Symptomatic +
loosening: full component revision.
• Component: Aligned: Head/liner exchange. Mal-positioned: complete
revision.
• Acetabular Rim: Supportive / Partially supportive: standard cup
(hemispherical) with multi-holes or high porous metal +/- augments
or cement to ↑ stability. Unsupportive (implant rock up and roll out
posteriorly or roll up and in) → superior medial defect: special
implants (Triflange cup, or cup-cage).
Subsidence of implant with
shortening and proximal
migration of GT.
Aseptic loosening
proximally
Gruen zones of
osteolysis: 3 acetabular &
7 femoral
27.
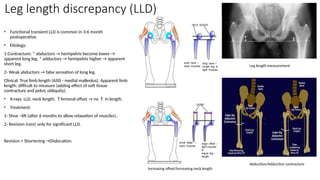
Leg length discrepancy(LLD)
• Functional transient LLD is common in 3-6 month
postoperative.
• Etiology:
1-Contracture: * abductors → hemipelvis become lower →
apparent long leg, * adductors → hemipelvis higher → apparent
short leg.
2- Weak abductors → false sensation of long leg.
Clinical: True limb length (ASIS - medial malleolus). Apparent limb
length: difficult to measure (adding effect of soft tissue
contracture and pelvic obliquity).
• X-rays: LLD, neck length. ↑femoral offset → no ↑ in length.
• Treatment:
1- Shoe –lift (after 6 months to allow relaxation of muscles)..
2- Revision (rare) only for significant LLD.
Revision + Shortening →Dislocation.
Abduction/Adduction contracture
Leg length measurement
Increasing offset/Increasing neck length
28.
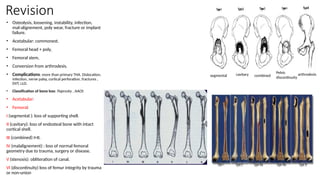
Revision
• Osteolysis, loosening,instability, infection,
mal-alignement, poly wear, fracture or implant
failure.
• Acetabular: commonest.
• Femoral head + poly,
• Femoral stem,
• Conversion from arthrodesis.
• Complications: more than primary THA. Dislocation,
infection, nerve palsy, cortical perforation, fractures ,
DVT, LLD.
• Classification of bone loss: Paprosky , AAOS
• Acetabular:
• Femoral:
I (segmental ): loss of supporting shell.
II (cavitary): loss of endosteal bone with intact
cortical shell.
III (combined) I+II.
IV (malalignement) : loss of normal femoral
geometry due to trauma, surgery or disease.
V (stenosis): obliteration of canal.
VI (discontinuity) loss of femur integrity by trauma
or non-union
cavitary
segmental combined
Pelvic
discontinuity
arthrodesis
29.
Revision
• Pain: groin(acetabulum), thigh (femoral stem),
start-up pain (loosening), night pain (infection)
• X-rays : AP, lateral , Judet views.
• CT scan: extent of osteolysis.
• ESR, CRP, CBC, Joint aspiration.
• Femoral revision:
• Paprosky – I: primary hip component.
• Pap – II, IIIa: Uncemented extensively porous
coated long stem or modular tapered stem (95%
survival rate at 10 years)…
• Pap – IIIb, IV: impaction bone graft for large ectatic
canal and thin cortices. Stem subsidence occurs.
• Pap – IV: allograft prosthetic component.
• Pap – IV with massive bone loss + non-supportive
diaphysis: Modular oncology prosthesis.
• Cemented stem for elderly, low demand, and
irradiated bone (high failure rate)
Extensively porous coated
long stem prosthesis
Modular oncology
prosthesis
Cemented stem Allograft cortical strut secured with
cercelage
30.
Revision
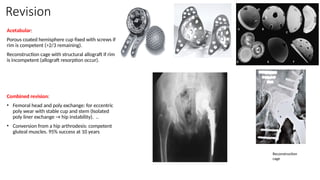
Acetabular:
Porous coated hemispherecup fixed with screws if
rim is competent (>2/3 remaining).
Reconstruction cage with structural allograft if rim
is incompetent (allograft resorption occur).
Combined revision:
• Femoral head and poly exchange: for eccentric
poly wear with stable cup and stem (Isolated
poly liner exchange → hip instability). ..
• Conversion from a hip arthrodesis: competent
gluteal muscles. 95% success at 10 years
Reconstruction
cage
31.
Revision
Revision total hiparthroplasty with use of a cemented femoral component. Results at a mean of ten years.
• Haydon CM, Mehin R, Burnett S, Rorabeck CH, Bourne RB, McCalden RW, MacDonald SJ. J Bone Joint Surg Am. 2004 Jun;86-A(6):1179-85.
• The results of 129 revision total hip arthroplasties that had been performed with use of a cemented femoral stem were reviewed to determine component survival.
Ninety-seven hips that had been followed for a minimum of five years were included in survival analysis and tests of significance. Harris hip scores were used to
quantify clinical outcomes. Clinical and surgical factors were analyzed to determine whether they were predictive of failure. RESULTS: The mean Harris hip score
improved from 52 points preoperatively to 71 points at the time of the most recent follow-up (p < 0.001). The ten-year survival rate was 91% with rerevision of the
femoral component because of aseptic loosening as the end point and 71% with mechanical failure as the end point. Patients who were more than sixty years old
had greater long-term component survival and less pain than younger patients did (p < 0.05). A good-quality postoperative cement mantle was associated with
better long-term radiographic signs of fixation (p < 0.001). Poor femoral bone quality was associated with an increased rate of rerevision for aseptic loosening (p =
0.021). CONCLUSIONS: Revision with use of a cemented femoral component remains an option for selected patients, with an acceptable ten-year survival rate and
fair radiographic evidence of fixation. Our patients had acceptable clinical outcomes at ten years, and few had notable pain. The best results may be achieved in older
patients (those who are sixty years old or more) with adequate bone stock who are managed with modern cementing techniques.
Revision total hip arthroplasty: the limits of fully coated stems.
• Sporer SM, Paprosky WG. Clin Orthop Relat Res. 2003 Dec;(417):203-9
• Femoral revision with a 7-inch or 8-inch fully porous-coated stem may not provide reliable long-term results in patients with moderate bone loss. The purpose of this
study was to evaluate the limits of fully porous-coated stems and to create a treatment algorithm for femoral deficiencies. Fifty-one patients with either a 10-inch or
9-inch calcar fully porous-coated stem, 10 patients with impaction bone grafting, and 10 patients with a modular tapered stem were evaluated at an average 4.2
years postoperatively. The mechanical failure rate among the 9-inch and 10-inch fully porous-coated stems was 0% in Type III B defects with femoral canals less than
19 mm (15 patients), 18% in Type IIIB defects with femoral canals greater than 19 mm (2 of 11 patients) and 37.5% in Type IV defects (three of eight patients). There
were no mechanical failures observed among the bone packing or modular tapered stems. Patients with Type IIIB defects and a femoral canal less than 19 mm can be
treated successfully with either a 10-inch or 9-inch calcar fully porous-coated stem. However, patients with Type IIIB defect and an endosteal canal greater than 19
mm or a Type IV defect require alternative methods of reconstruction such as a modular tapered stem or a bone packing procedure.
Results
Cement-in-cement femoral componentrevision in the multiply revised total hip arthroplasty results with a minimum follow-up of five years
N. A. Sandiford, S. S. Jameson, M. J. Wilson, M. J. W. Hubble, A. J. Timperley, J. R. Howell . Bone Joint J 2017;99-B:199–203.
Aims We present the clinical and radiological results at a minimum follow-up of five years for patients who have undergone multiple cement-in-cement revisions of their femoral
component at revision total hip arthroplasty (THA). Patients and Methods We reviewed the outcome on a consecutive series of 24 patients (10 men, 14 women) (51 procedures) who
underwent more than one cement-in-cement revision of the same femoral component. The mean age of the patients was 67.5 years (36 to 92) at final follow-up. Function was assessed
using the original Harris hip score (HHS), Oxford Hip Score (OHS) and the Merle D’Aubigné Postel score (MDP). Results The mean length of follow-up was 81.7 months (64 to 240). A
total of 41 isolated acetabular revisions were performed in which stem removal facilitated access to the acetabulum, six revisions were conducted for loosening of both components
and two were isolated stem revisions (each of these patients had undergone at least two revisions). There was significant improvement in the OHS (p = 0.041), HHS (p = 0.019) and
MDP (p = 0.042) scores at final follow-up There were no stem revisions for aseptic loosening. Survival of the femoral component was 91.9% (95% confidence intervals (CI) 71.5 to 97.9)
at five years and 91.7% (95% CI 70 to 97) at ten years (number at risk 13), with stem revision for all causes as the endpoint. Conclusion Cement-in-cement revision is a viable technique
for performing multiple revisions of the well cemented femoral component during revision total hip arthroplasty at a minimum of five years follow-up.
Ceramic-on-ceramic bearing fractures in total hip arthroplasty, an analysis of data from the National Joint Registry
D. P. Howard, P. D. H. Wall, M. A. Fernandez, H. Parsons, P. W. Howard. Bone Joint J 2017;99-B:1012–19.
Aims Ceramic-on-ceramic (CoC) bearings in total hip arthroplasty (THA) are commonly used, but concerns exist regarding ceramic fracture. This study aims to report
the risk of revision for fracture of modern CoC bearings and identify factors that might influence this risk, using data from the National Joint Registry (NJR) for
England, Wales, Northern Ireland and the Isle of Man. Patients and Methods We analysed data on 223 362 bearings from 111 681 primary CoC THAs and 182 linked
revisions for bearing fracture recorded in the NJR. We used implant codes to identify ceramic bearing composition and generated Kaplan-Meier estimates for implant
survivorship. Logistic regression analyses were performed for implant size and patient specific variables to determine any associated risks for revision. Results A total
of 222 852 bearings (99.8%) were CeramTec Biolox products. Revisions for fracture were linked to seven of 79 442 (0.009%) Biolox Delta heads, 38 of 31 982 (0.119%)
Biolox Forte heads, 101 of 80 170 (0.126%) Biolox Delta liners and 35 of 31 258 (0.112%) Biolox Forte liners. Regression analysis of implant size revealed smaller
heads had significantly higher odds of fracture (chi-squared 68.0, p < 0.001). The highest fracture risk was observed in the 28 mm Biolox Forte subgroup (0.382%).
There were no fractures in the 40 mm head group for either ceramic type. Liner thickness was not predictive of fracture (p = 0.67). Body mass index (BMI) was
independently associated with revision for both head fractures (odds ratio (OR) 1.09 per unit increase, p = 0.031) and liner fractures (OR 1.06 per unit increase,
p = 0.006). Conclusions We report the largest independent study of CoC bearing fractures to date. The risk of revision for CoC bearing fracture is very low but
previous studies have underestimated this risk. There is good evidence that the latest generation of ceramic has greatly reduced the odds of head fracture but not of
liner fracture. Small head size and high patient BMI are associated with an increased risk of ceramic bearing fracture.
34.
Results
A 28-year clinicaland radiological follow-up of alumina ceramic-on-crosslinked polyethylene total hip arthroplasty a follow-up report and analysis of the
oxidation of a shelf-aged acetabular component.
A. Rajpura, T. N. Board, P. D. Siney, H. Wynn Jones, S. Williams, L. Dabbs, B. M. Wroblewski. Bone Joint J 2017;99-B:1286–9.
Aims Our aim in this study was to describe a continuing review of 11 total hip arthroplasties using 22.225 mm Alumina ceramic femoral heads on a Charnley flanged
femoral component, articulating against a silane crosslinked polyethylene.
Patients and Methods Nine patients (11 THAs) were reviewed at a mean of 27.5 years (26 to 28) post-operatively. Outcome was assessed using the d’Aubigne and
Postel, and Charnley scores and penetration was recorded on radiographs. In addition, the oxidation of a 29-year-old shelf-aged acetabular component was analysed.
Results The mean clinical outcome scores remained excellent at final follow-up. The mean total penetration remained 0.41 mm (0.40 to 0.41). There was no
radiographic evidence of acetabular or femoral loosening or osteolysis. There was negligible oxidation in the shelf-aged sample despite gamma irradiation and storage
in air. Conclusion These results highlight the long-term stability and durability of this type of crosslinked, antioxidant containing polyethylene when used in
combination with a small diameter alumina ceramic femoral head.
Risk of early mortality after cemented compared with cementless total hip arthroplasty, a nationwide matched cohort study
A. Garland, M. Gordon, G. Garellick, J. Kärrholm, O. Sköldenberg, N. P. Hailer. Bone Joint J 2017;99-B:37–43.
Aims It has been suggested that cemented fixation of total hip arthroplasty (THA) is associated with an increased peri-operative mortality compared with cementless
THA. Our aim was to investigate this through a nationwide matched cohort study adjusting for age, comorbidity, and socioeconomic background.
Patients and Methods A total of 178 784 patients with osteoarthritis who underwent either cemented or cementless THA from the Swedish Hip Arthroplasty Register
were matched with 862 294 controls from the general population. Information about the causes of death, comorbidities, and socioeconomic background was
obtained. Mortality within the first 90 days after the operation was the primary outcome measure. Results Patients who underwent cemented THA had an increased
risk of death during the first 14 days compared with the controls (hazard ratio (HR) 1.3, confidence interval (CI) 1.11 to 1.44), corresponding to an absolute increase in
risk of five deaths per 10 000 observations. No such early increase of risk was seen in those who underwent cementless THA. Between days 15 and 29 the risk of
mortality was decreased for those with cemented THA (HR 0.7, CI 0.62 to 0.87). Between days 30 and 90 all patients undergoing THA, irrespective of the mode of
fixation, had a lower risk of death than controls. Patients selected for cementless fixation were younger, healthier and had a higher level of education and income than
those selected for cemented THA. A supplementary analysis of 16 556 hybrid THAs indicated that cementation of the femoral component was associated with a slight
increase in mortality up to 15 days, whereas no such increase in mortality was seen in those with a cemented acetabular component combined with a cementless
femoral component. Conclusion This nationwide matched cohort study indicates that patients receiving cemented THA have a minimally increased relative risk of early
mortality that is reversed from day 15 and thereafter. The absolute increase in risk is very small. Our findings lend support to the idea that cementation of the femoral
component is more dangerous than cementation of the acetabular component.
35.
Summary
Hip surgery –state of the art
Totally Hip 2017: Gothenburg
A. R. J. Manktelow, T. Gehrke, F.
S. Haddad. BJJ-2017-0188 Published 31
March 2017
The operation of the century: total hip replacement
Prof Ian D Learmonth, Claire Young, FRCS, Prof Cecil Rorabeck,
FRCS: 29 March 2007
In the 1960s, THR revolutionised management of elderly
patients crippled with arthritis, with very good long-term
results. Today, young patients present for hip-replacement
surgery hoping to restore their quality of life and physically
demanding activities.
Advances in bioengineering technology have driven
development of hip prostheses. Both cemented and
uncemented hips can provide durable fixation. Better
materials and design have allowed use of large-bore bearings,
which provide an increased range of motion with enhanced
stability and very low wear.
Minimally invasive surgery limits soft-tissue damage and
facilitates accelerated discharge and rehabilitation. Short-term
objectives must not compromise long-term performance.
Computer-assisted surgery will contribute to reproducible and
accurate placement of implants.
Further developments in total hip replacement will be
governed by their cost-effectiveness.