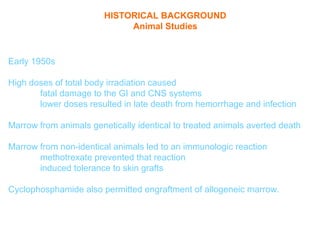
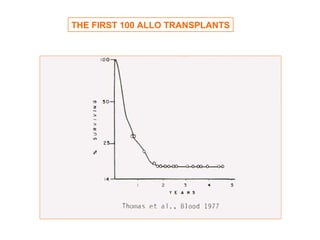
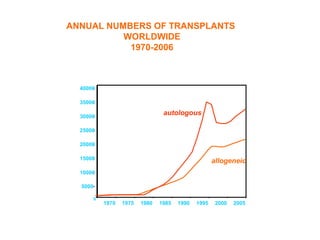
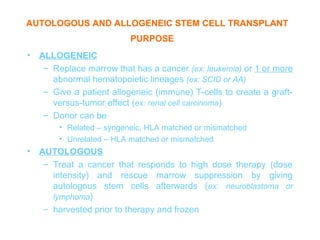
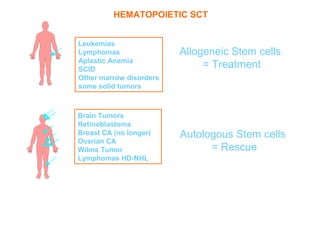
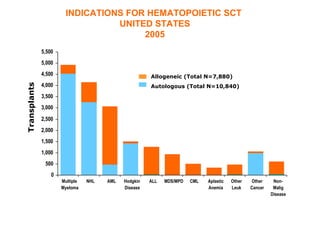
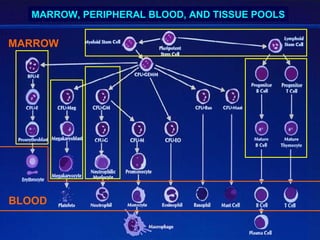
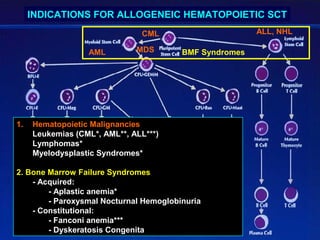
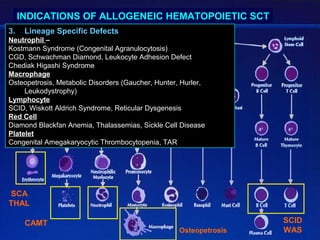
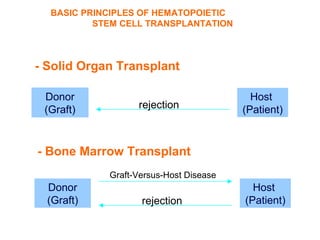
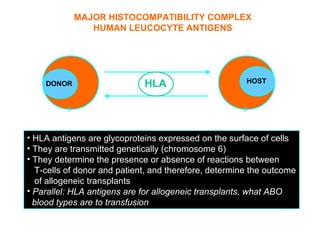
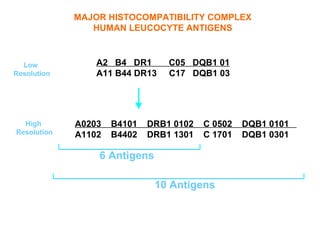
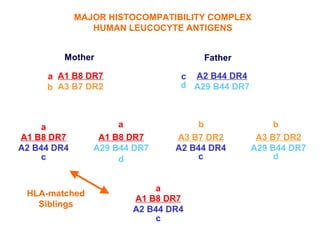
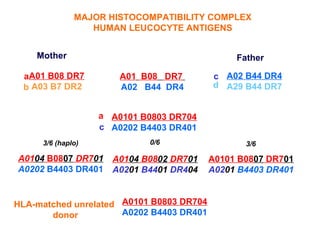
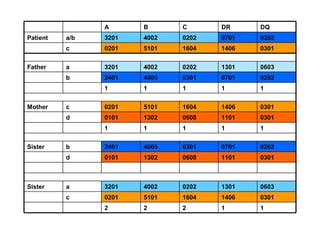
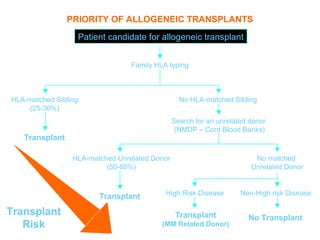
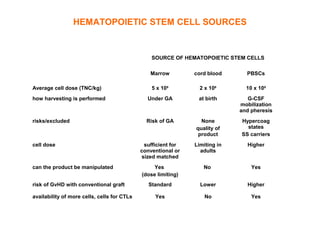
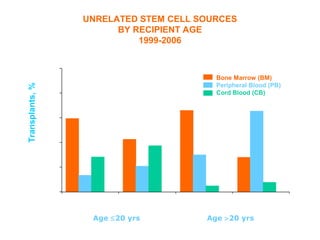
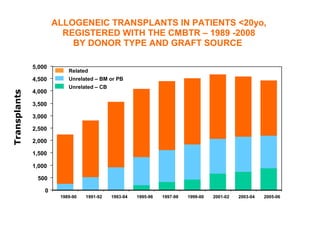
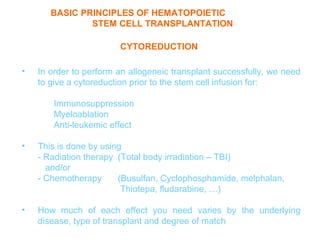
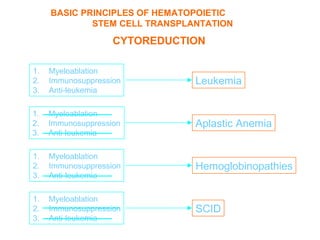
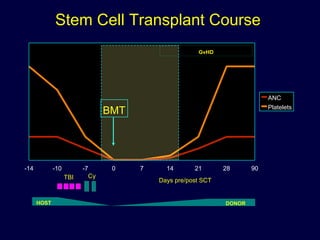
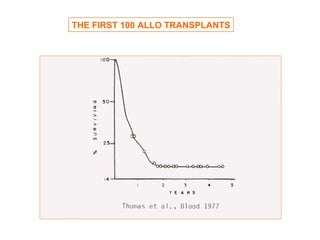
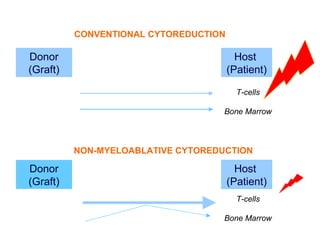
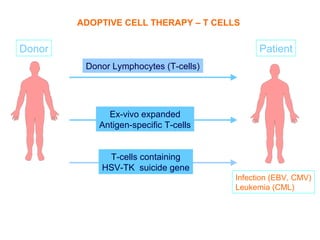
This document provides an overview of hematopoietic stem cell transplantation (HSCT) for pediatric patients with congenital or acquired hematopoietic disorders. It discusses the historical background of HSCT, including early animal studies and the first human transplants. It also covers the basic principles and indications for autologous and allogeneic HSCT, including the use of different stem cell sources like bone marrow, peripheral blood, and cord blood. Key factors like human leukocyte antigen matching between donor and recipient and the need for cytoreduction prior to transplant are also summarized.