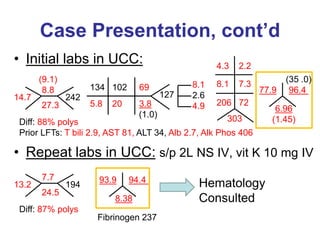
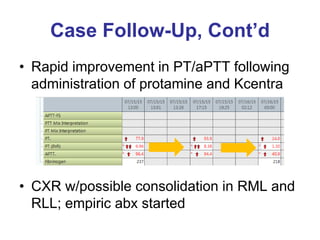
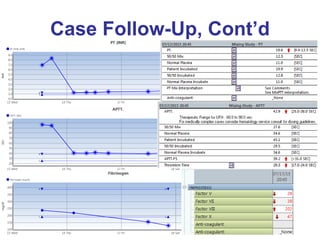
A 69-year-old man with metastatic pancreatic cancer presented with coagulopathy, hypotension, and melena. He had been receiving enoxaparin for DVT but now had markedly elevated PT and aPTT due to accumulation of enoxaparin from renal impairment, vitamin K deficiency from poor nutrition, and possible DIC. Hematology recommended administering protamine to reverse the effects of enoxaparin, 4-factor prothrombin complex concentrate to correct the coagulopathy, and continued vitamin K to address the deficiency. The patient's coagulopathy improved after these interventions but his renal function did not.