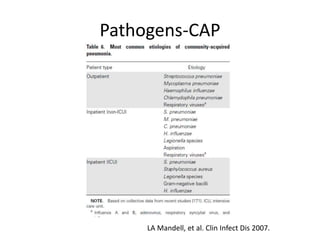
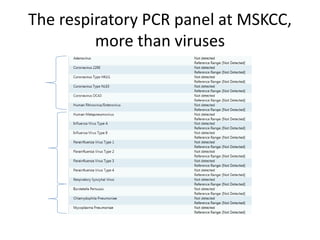
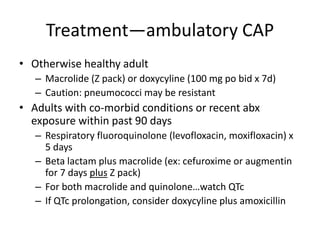
This document discusses various types and classifications of pneumonia, including community acquired pneumonia (CAP), hospital acquired pneumonia (HAP), healthcare associated pneumonia (HCAP), and ventilator-associated pneumonia (VAP). It then presents four clinical case studies of patients presenting with pneumonia and discusses the likely pathogens involved, appropriate testing, and treatment recommendations for each case. Key considerations included distinguishing between various pneumonia types and selecting initial empiric antibiotic therapy based on likely pathogens and patient risk factors or comorbidities.




































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)