Downloaded 523 times





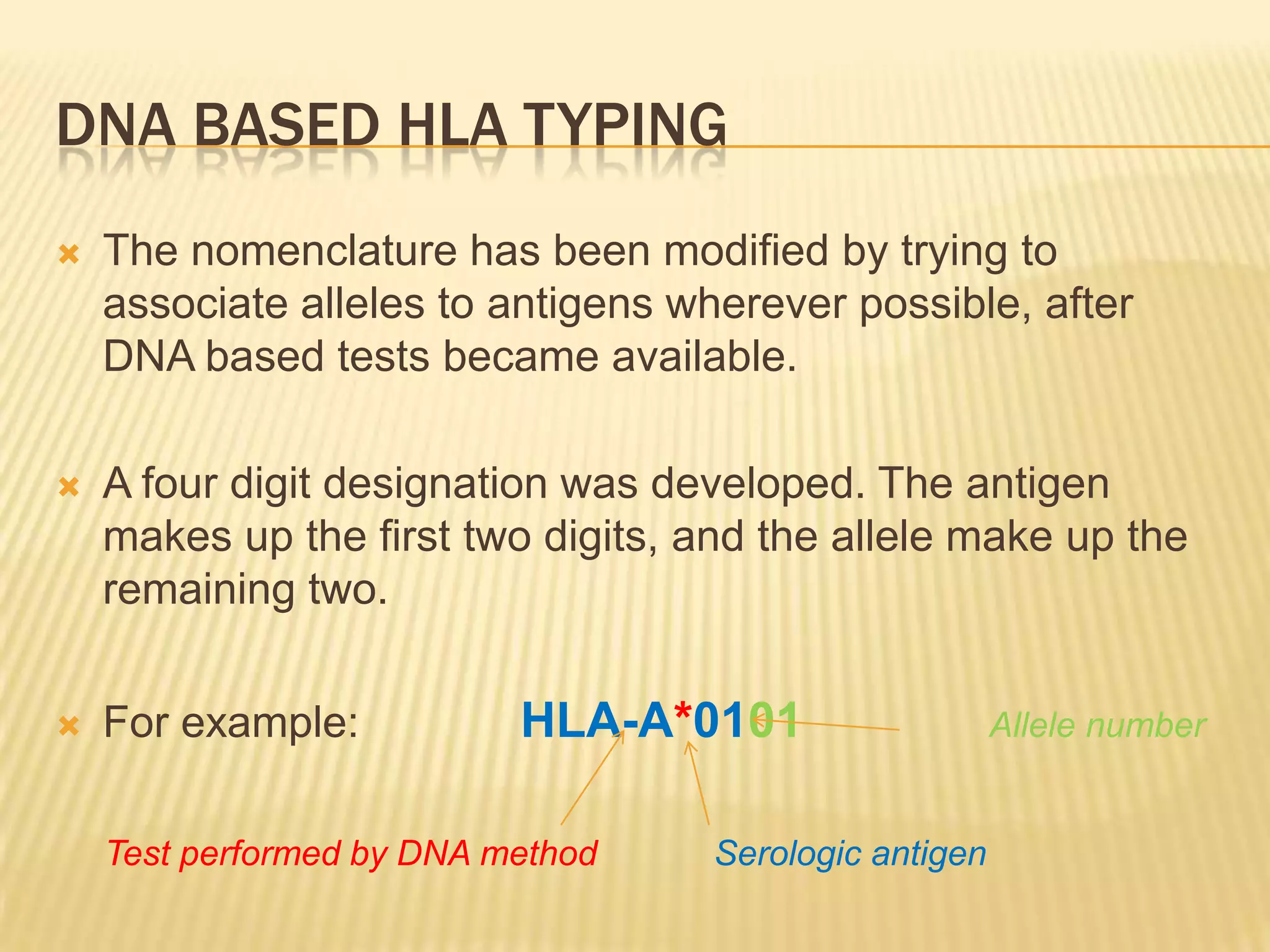






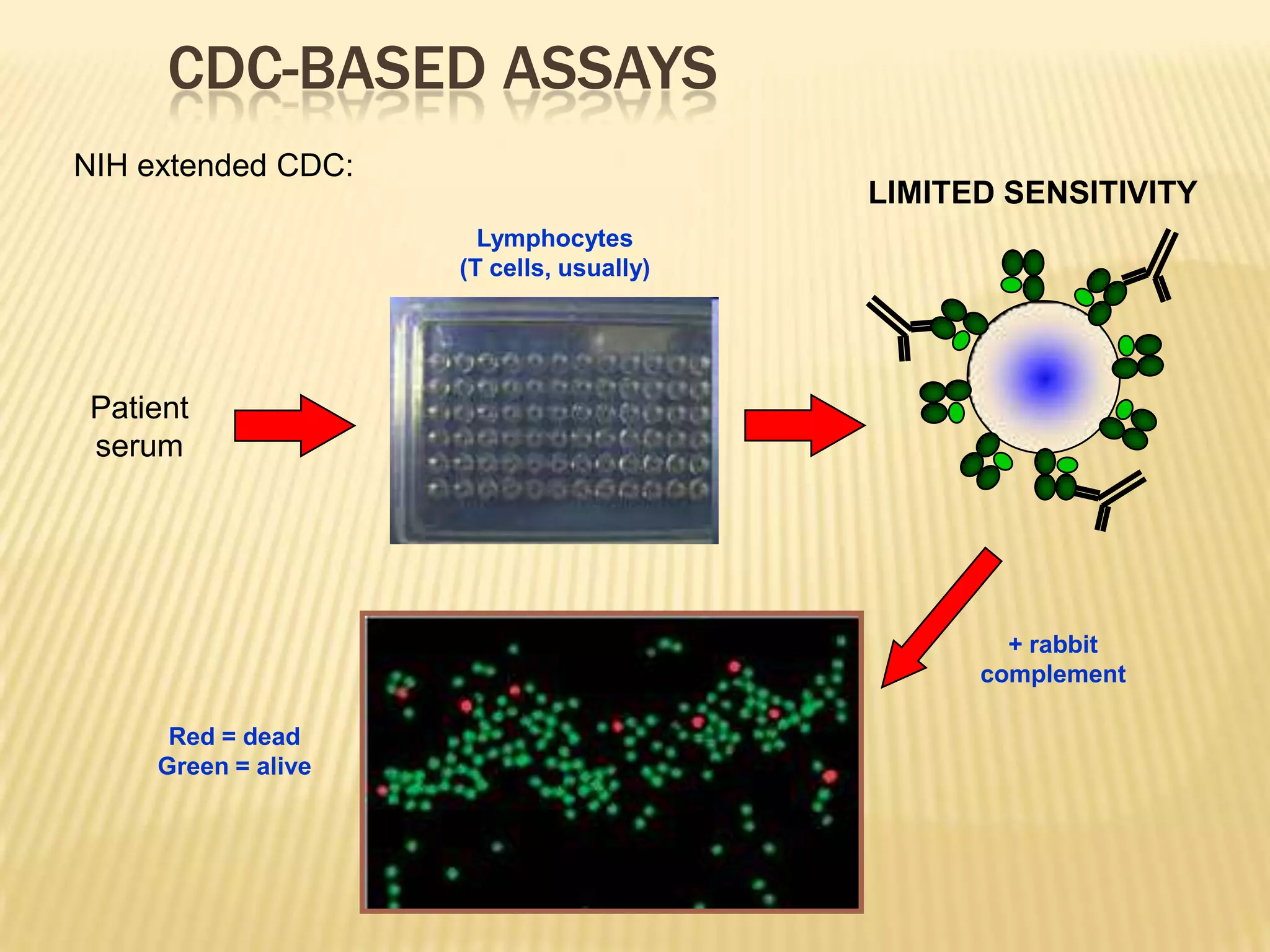

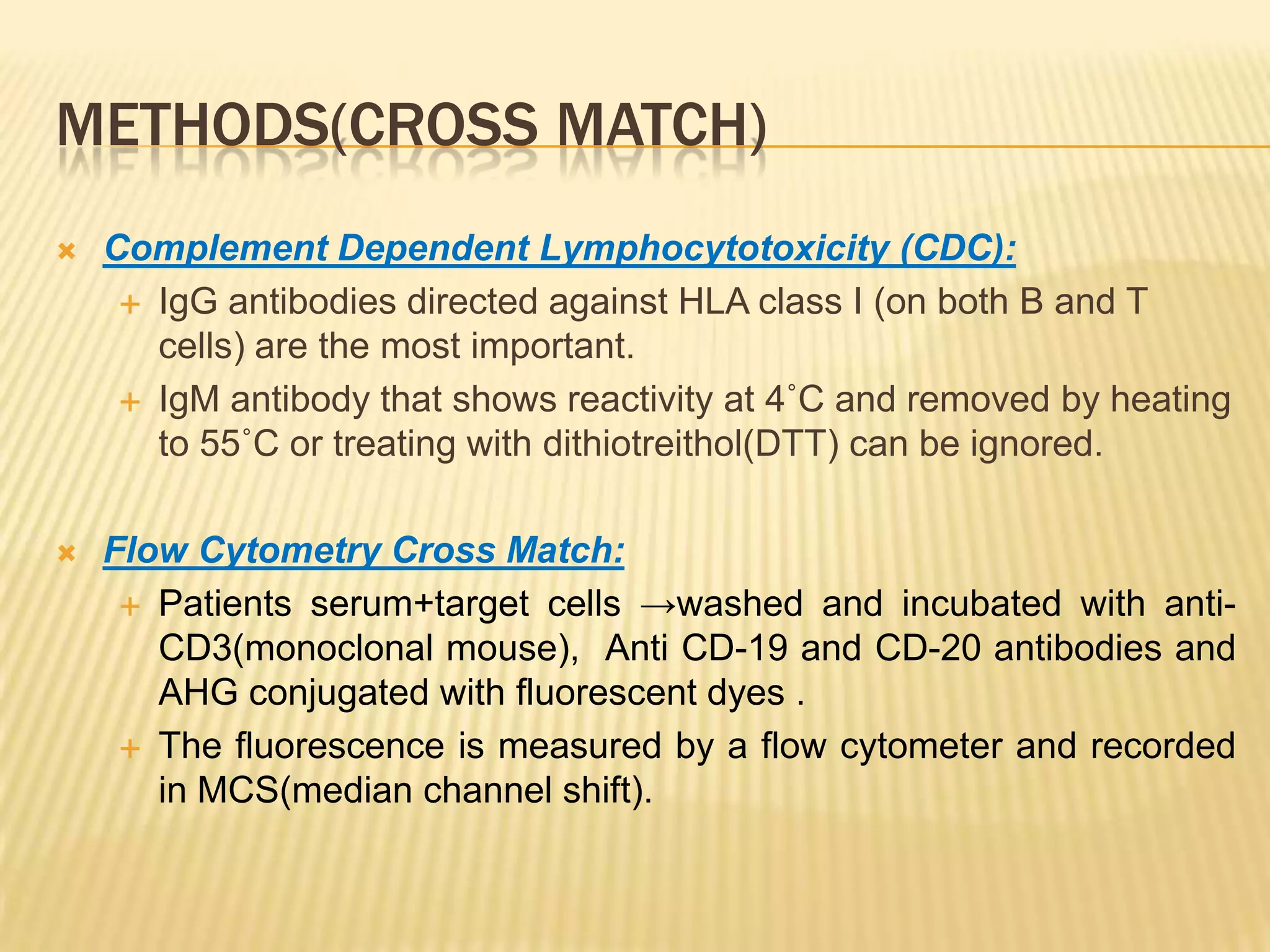


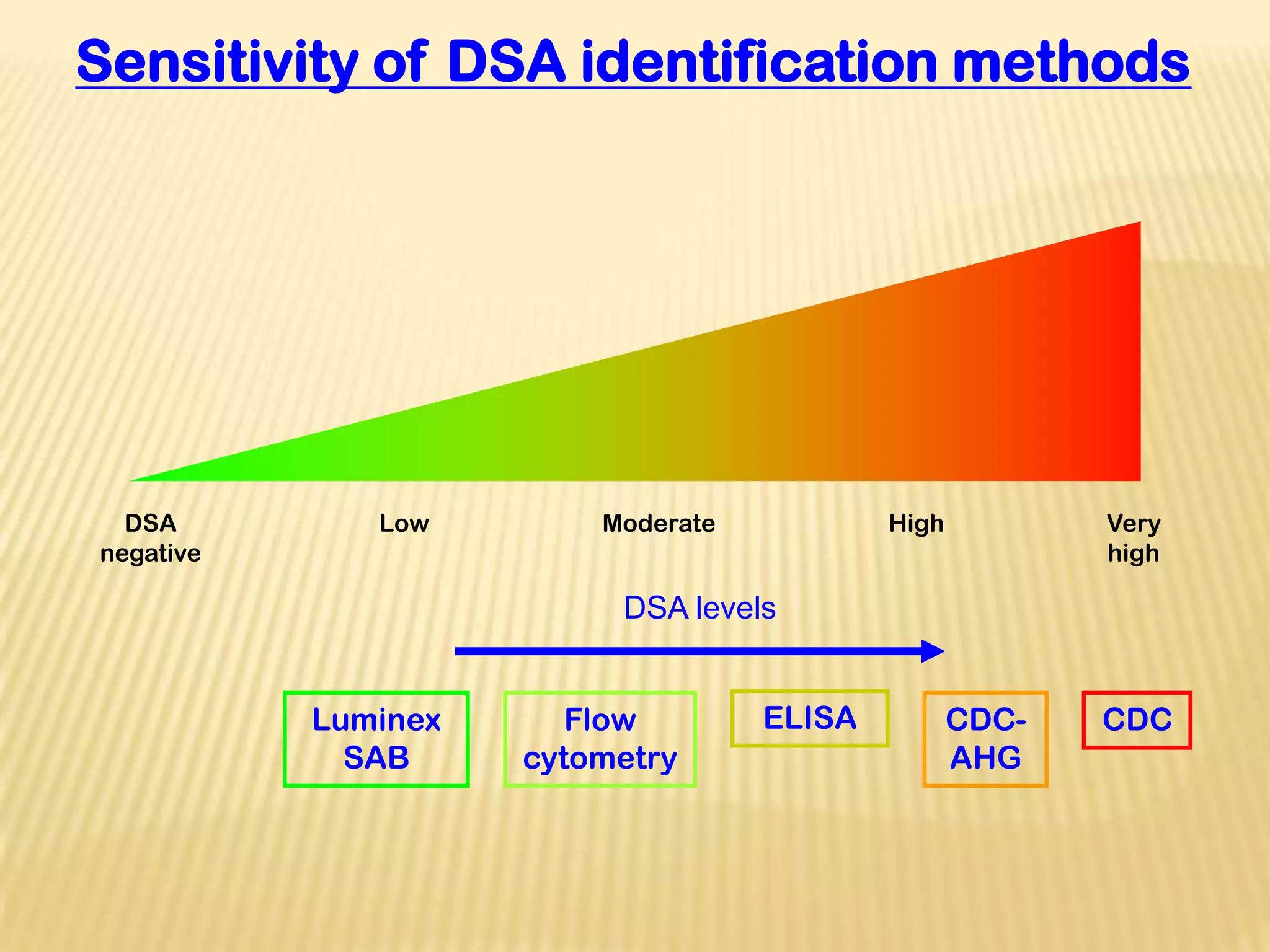














This document discusses HLA typing, crossmatching, and transplantation in sensitized patients. It begins with a brief history of organ transplantation. It then covers topics such as the structure and function of MHC molecules, methods of HLA typing including serological and DNA-based techniques, interpreting HLA typing reports, detecting sensitization through antibody detection tests, defining and identifying sensitized patients, and challenges in transplanting sensitized patients. Advances in diagnostics and therapeutics have helped increase transplantation options for sensitized patients.










































































































