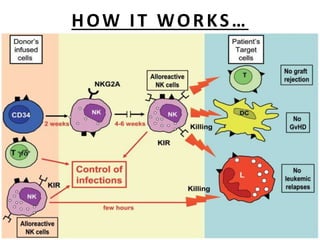
This document discusses the history and development of haploidentical stem cell transplantation. It begins with early research in the 1940s-1960s in mice and humans. Clinical haploidentical transplantation failed initially due to graft rejection. Advances included T-cell depletion to prevent graft-versus-host disease. More recent developments demonstrate sustained engraftment and reduced GVHD using purified donor T-cells and megadoses of granulocyte colony-stimulating factor. The role of total body irradiation conditioning is also summarized.