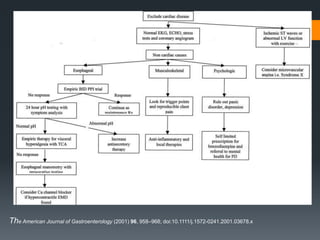
This document provides an overview of evaluating and managing chest pain. It discusses the many potential causes of chest pain including cardiac, pulmonary, gastrointestinal and psychiatric conditions. Key points include that up to 30% of cardiac catheterizations for suspected coronary artery disease are negative. The diagnostic workup involves considering the patient's history, symptoms, physical exam, ECG, cardiac biomarkers, imaging and ruling out life-threatening causes like aortic dissection and pulmonary embolism. For suspected acute coronary syndrome, treatment involves antiplatelet agents, anticoagulants, nitroglycerin, beta-blockers, oxygen and considering cardiac catheterization if within 90 minutes of symptoms.


















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















