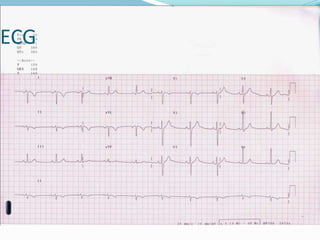
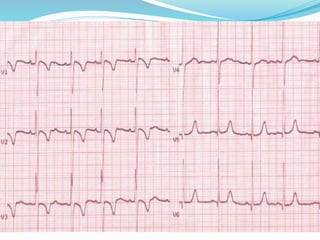
The document outlines the history, recording, and interpretation of electrocardiograms (ECGs), including the types of leads used and the physiological basis behind ECG waveforms. It discusses standard ECG measurement techniques and various cardiac conditions identifiable through ECG analysis, such as hypertrophy and arrhythmias. Key features like heart rate determination, axis alignment, and abnormal findings are highlighted to assist in clinical assessment.












































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















