Downloaded 26 times
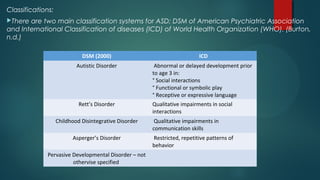
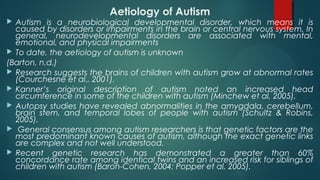
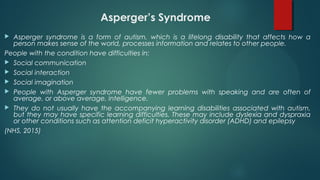
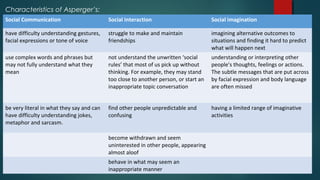

Autism Spectrum Disorder (ASD) encompasses a range of lifelong neurodevelopmental disabilities characterized by impairments in social communication and restricted behaviors, with recent DSM-5 updates consolidating prior diagnoses into a single category. The etiology remains largely unknown, though genetic factors are believed to play a significant role, alongside observed neurobiological anomalies. Various interventions, including behavioral and communicative strategies, aim to support individuals with ASD, particularly in managing co-occurring conditions such as ADHD.