Downloaded 3,645 times


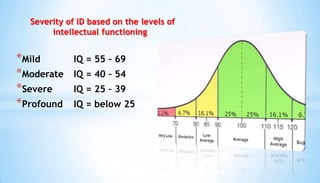

































Intellectual disability is characterized by deficits in cognitive ability and adaptive functioning that originate before age 18. It involves limitations in conceptual, social, and practical skills. The severity of intellectual disability can be mild, moderate, severe, or profound based on IQ scores. Causes include genetic syndromes, biological factors, medical conditions during pregnancy or birth, and psychosocial problems. Placement programs may include inclusion, individualized education, behavior therapy, and transition to adult services focusing on independent living skills and employment. Current research studies various approaches to improving academic engagement and quality of life for those with intellectual disability.