Downloaded 13 times
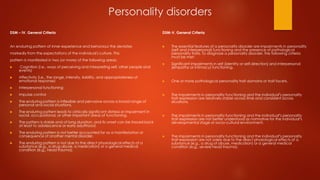
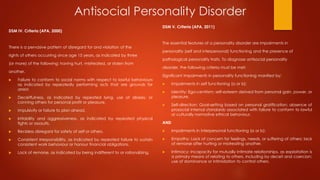

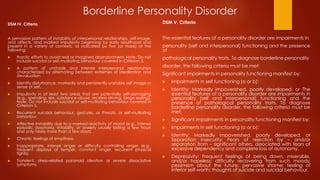

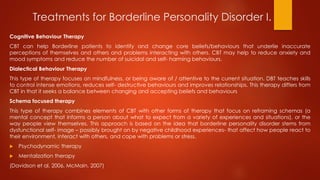


The document outlines the criteria for diagnosing personality disorders according to DSM-IV and DSM-V, emphasizing the importance of stable impairments in personality functioning and the presence of pathological traits. It specifically details the criteria for Antisocial and Borderline Personality Disorders, highlighting behaviors and patterns associated with each. Additionally, the document discusses various therapeutic approaches for treating Borderline Personality Disorder, including Cognitive Behavioral Therapy and Psychodynamic Therapy, while acknowledging the challenges faced in treatment.












































































