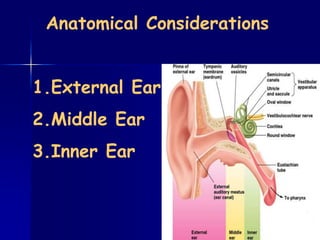
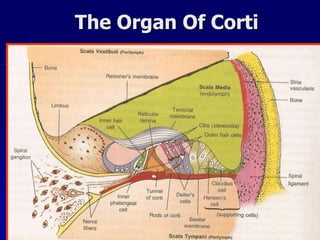
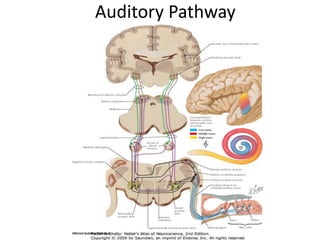
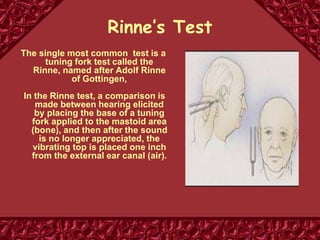
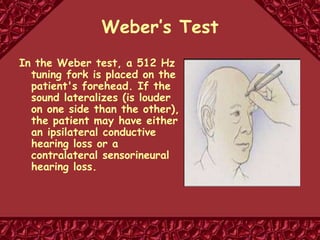
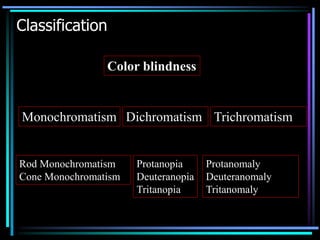
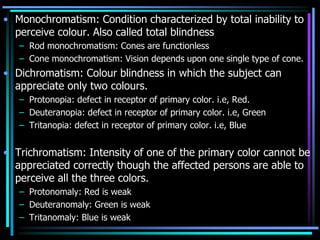
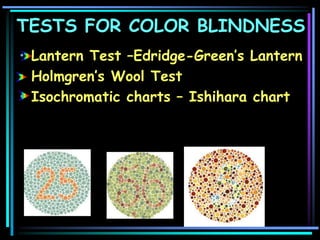
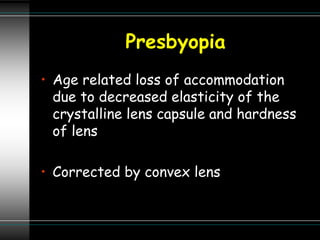
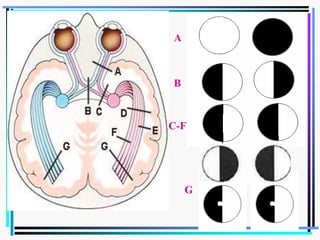
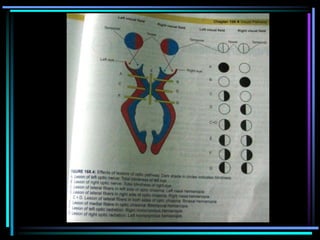
The document outlines the anatomy and functions of the auditory system, detailing the structures of the external, middle, and inner ear, as well as the auditory pathway from hair cells to the auditory cortex. It discusses types of deafness, including conductive and nerve deafness, along with their causes and testing methods, such as Rinne's and Weber's tests. Additionally, it covers color blindness, presbyopia, refractive errors, and lesions of the visual pathway.















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







