Downloaded 1,348 times

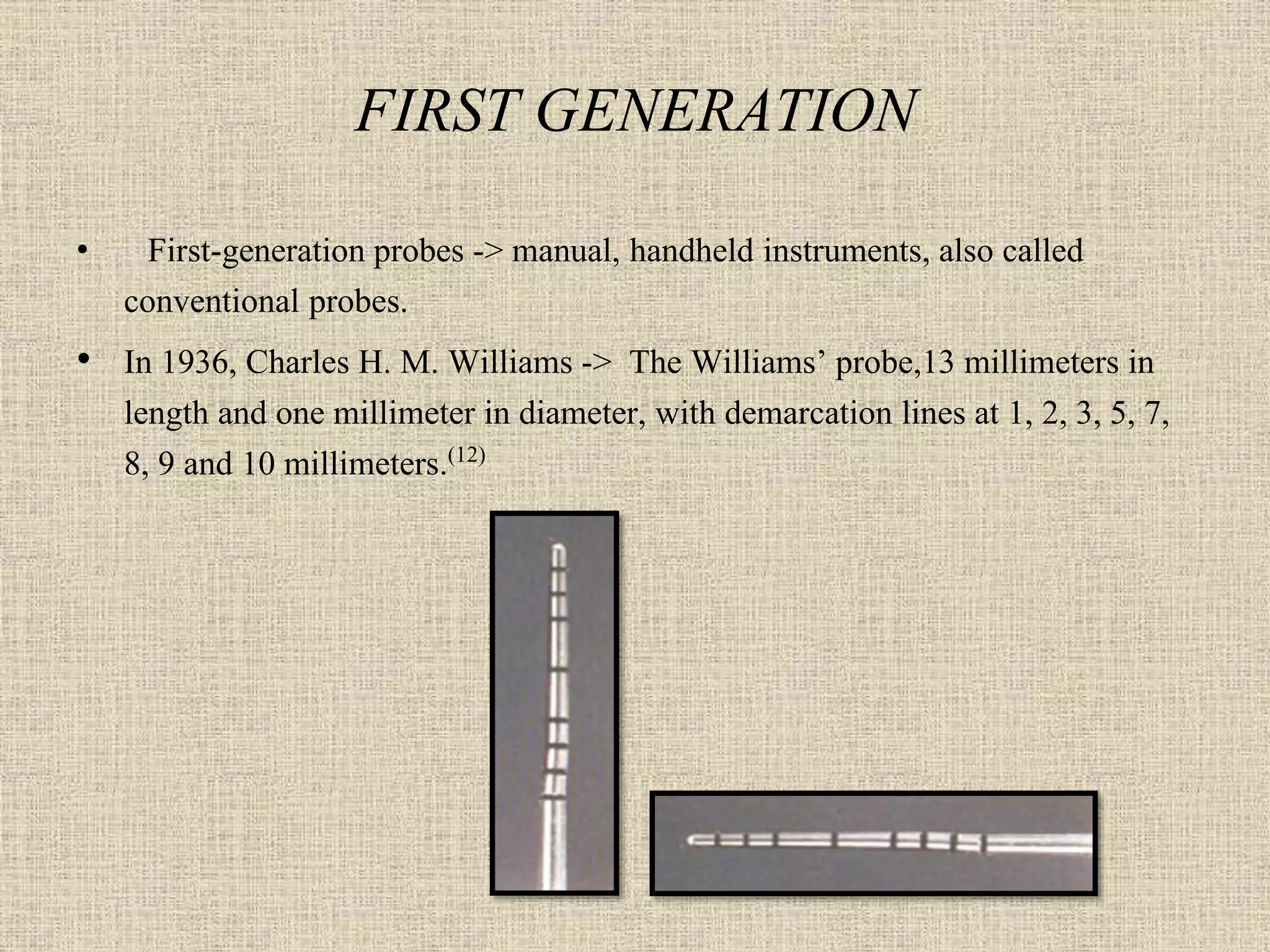



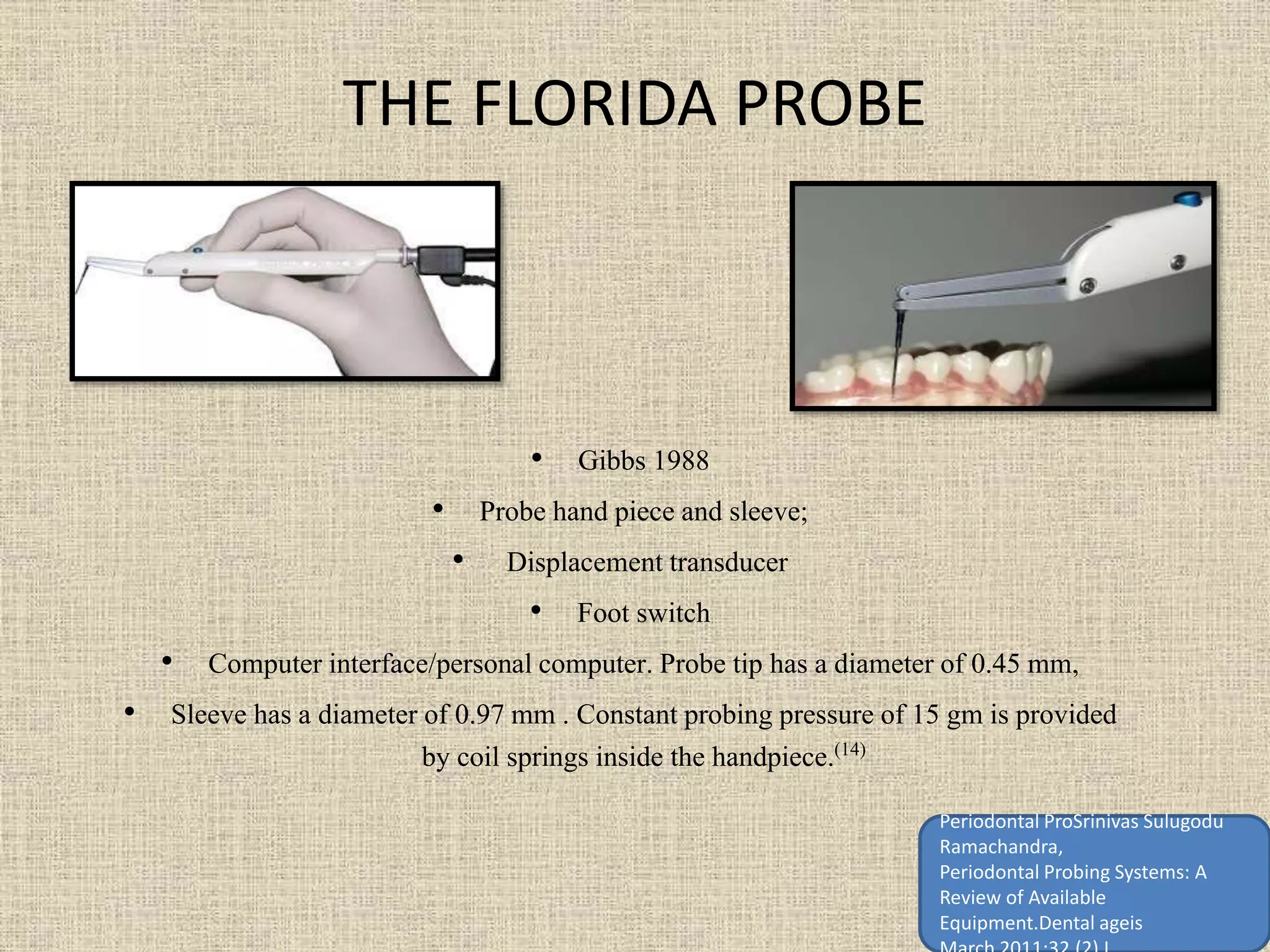







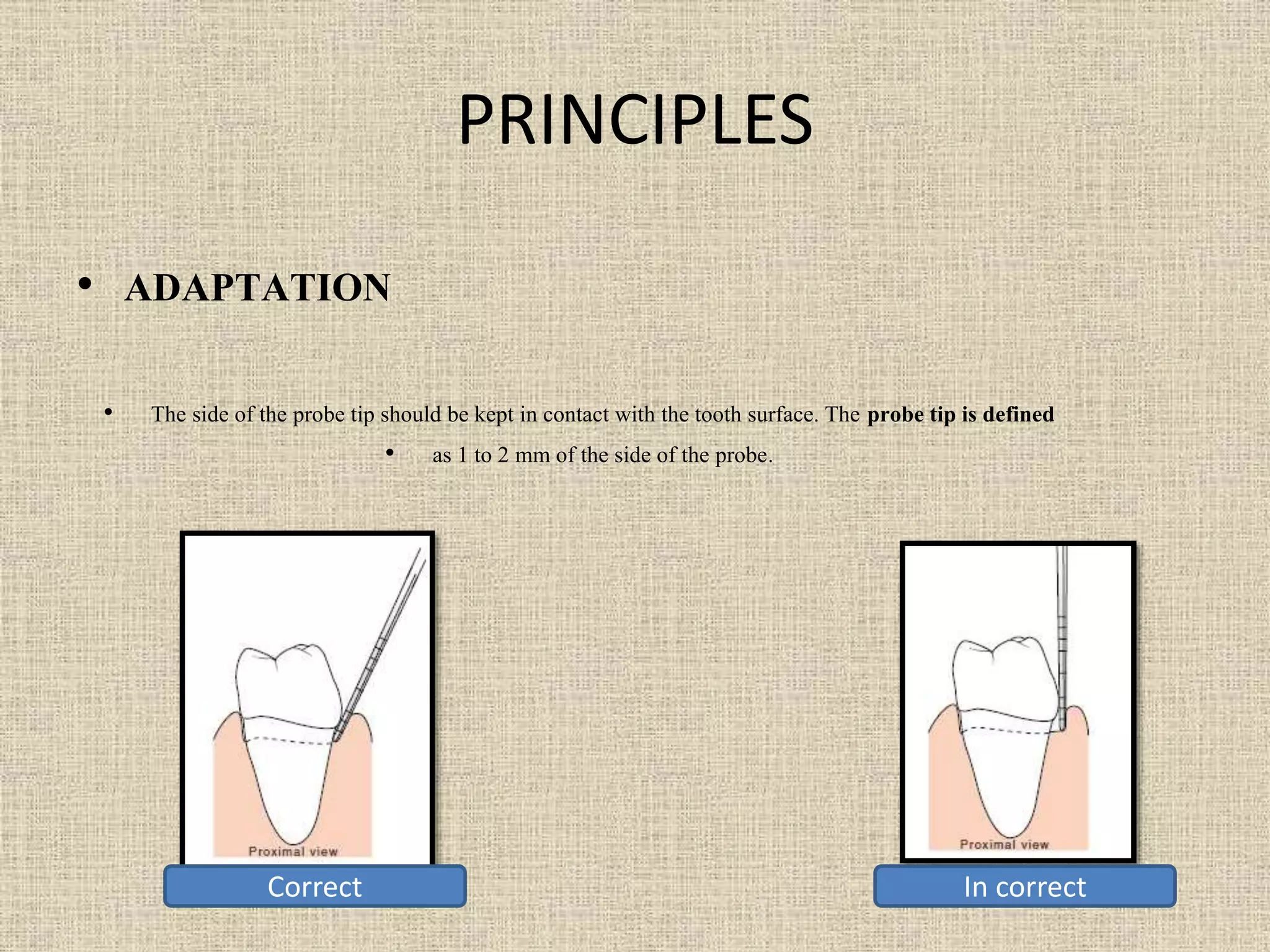
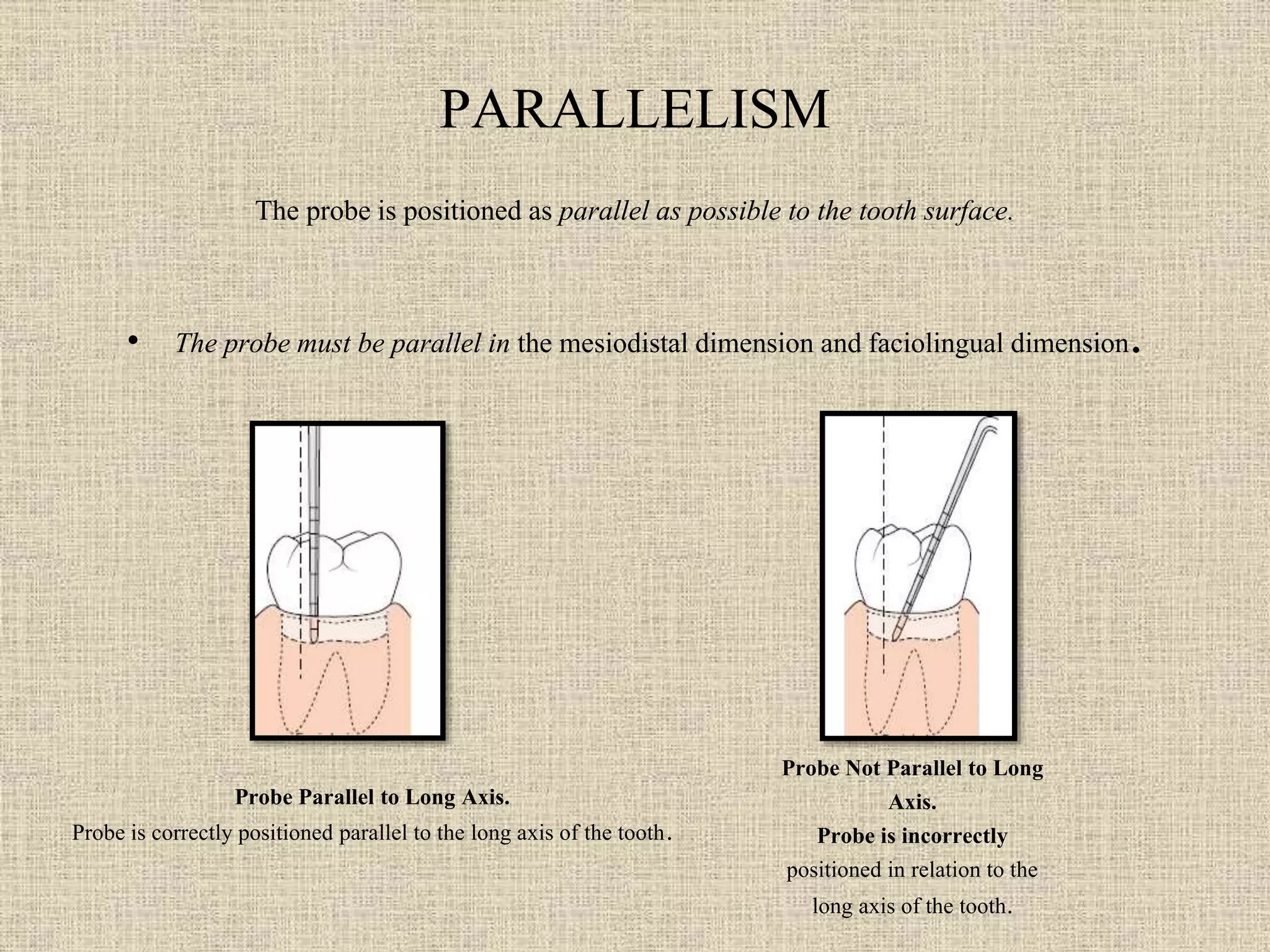
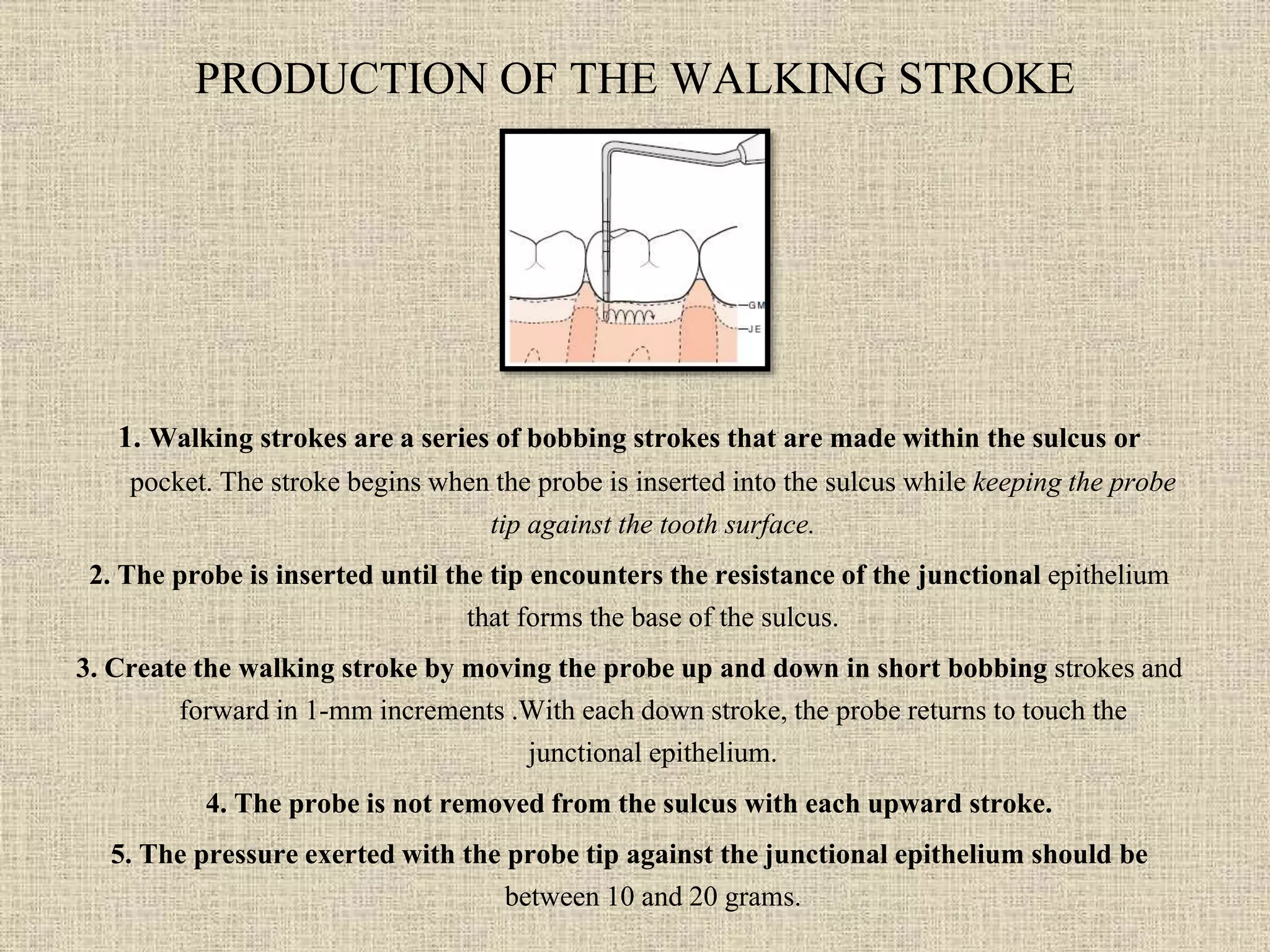
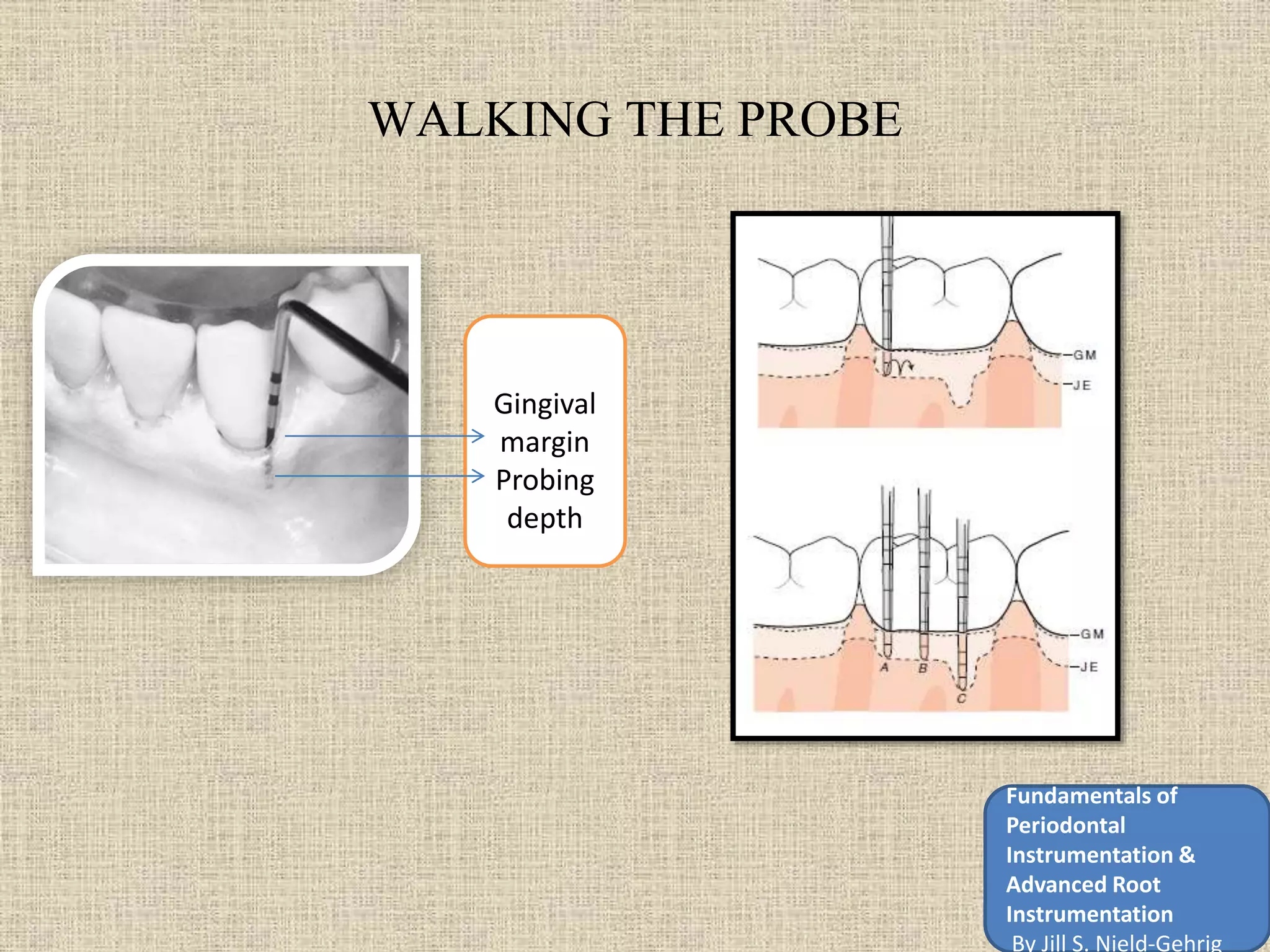
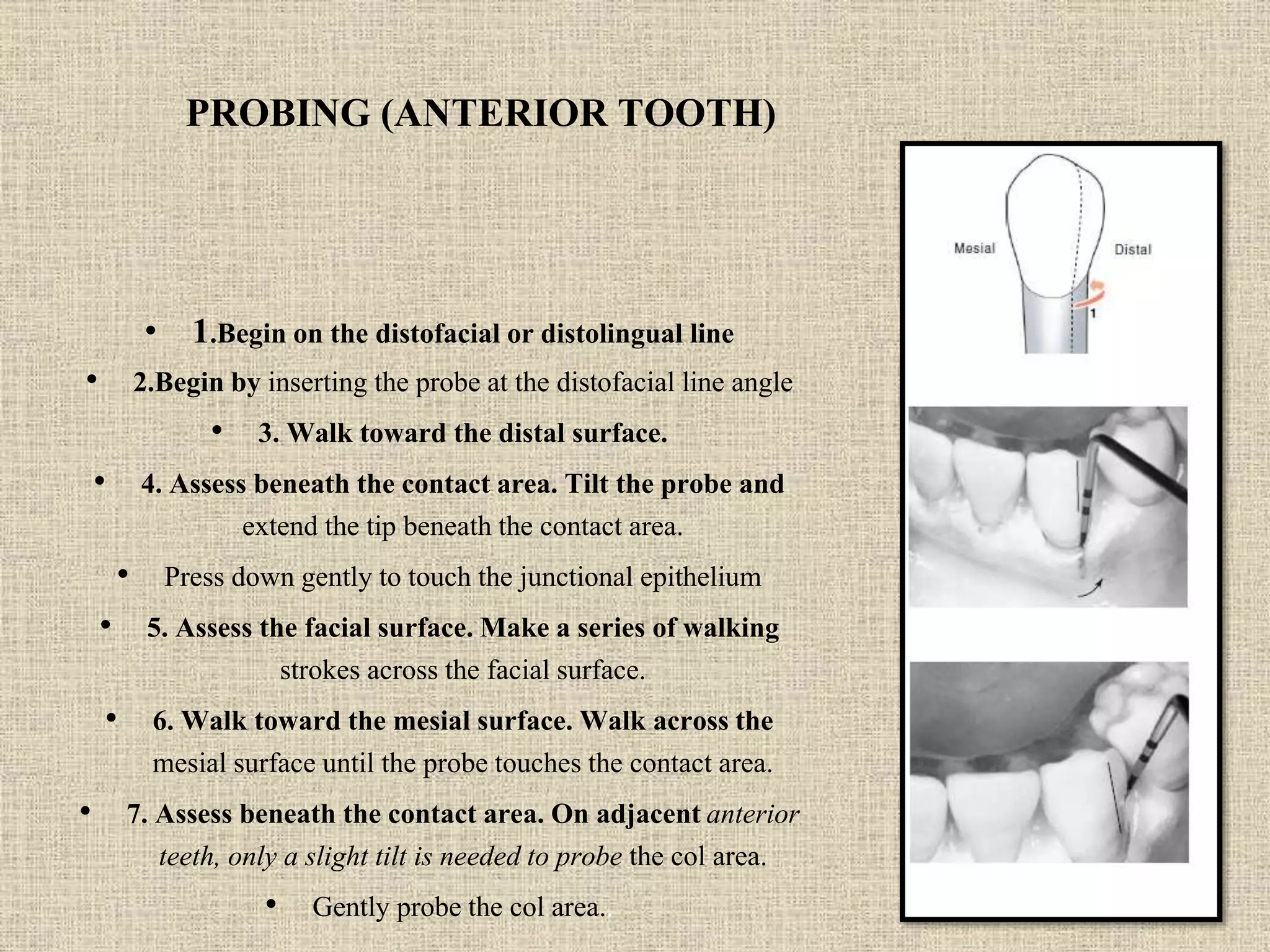
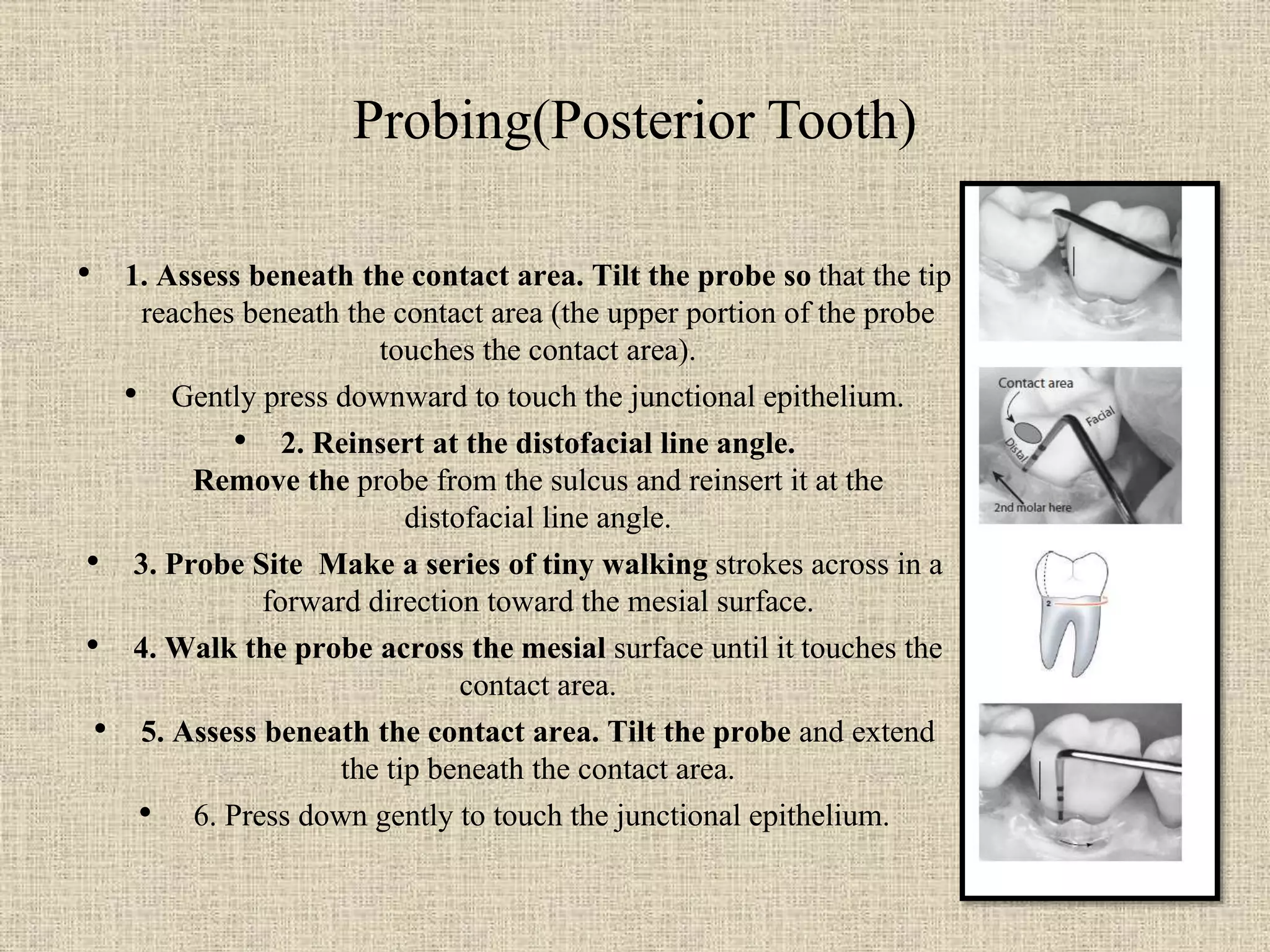


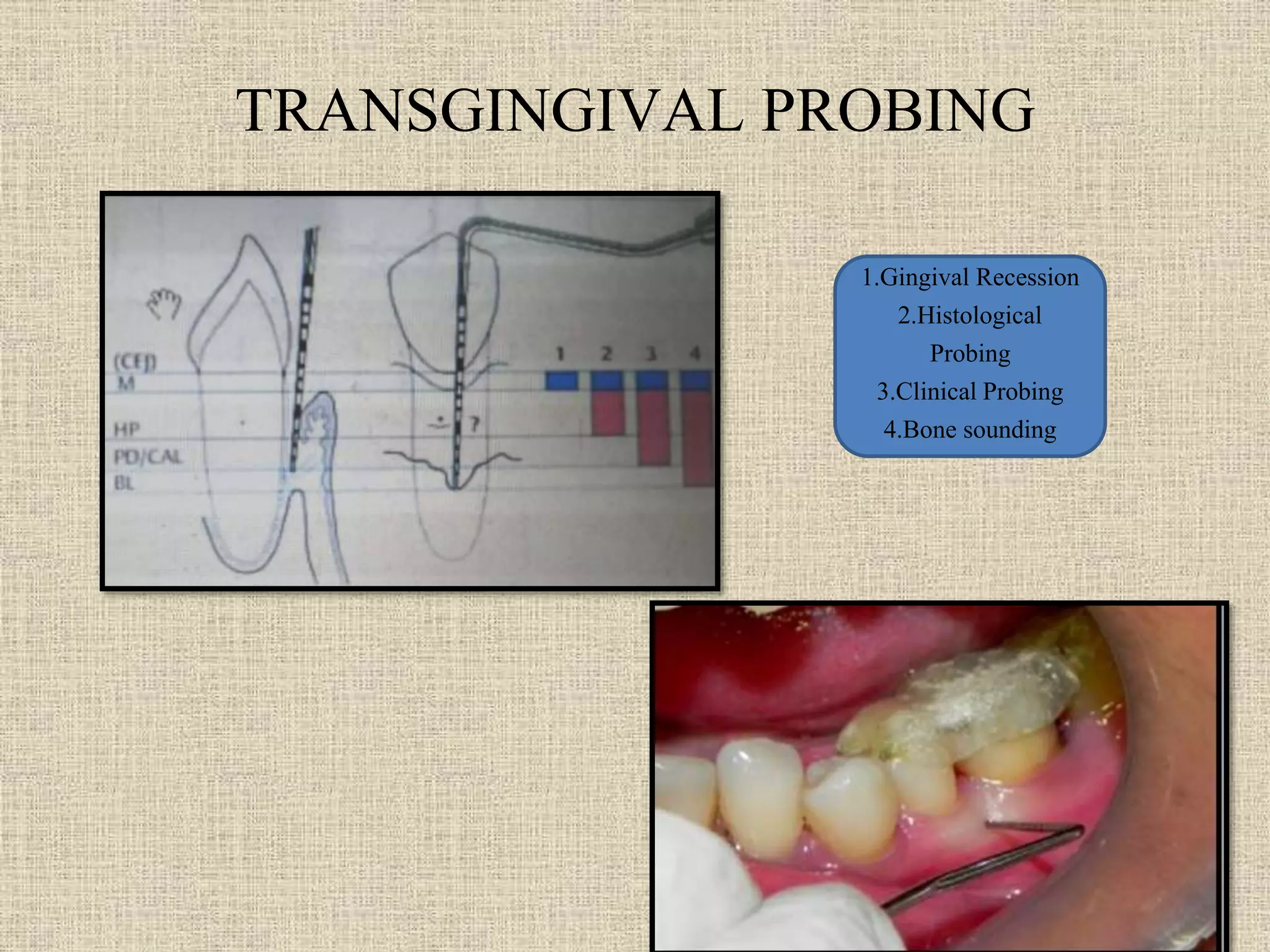
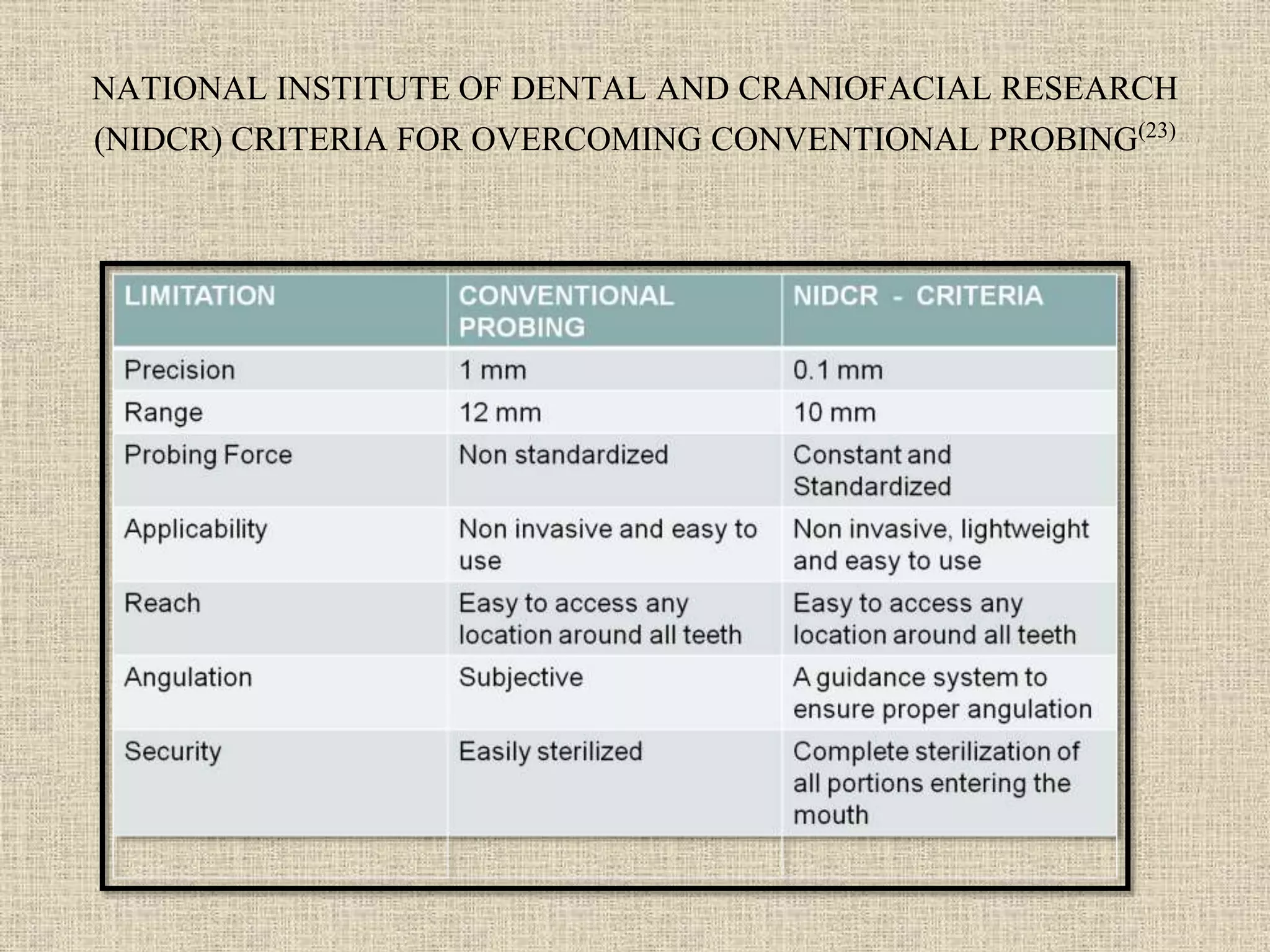










Periodontal probing and techniques involve using calibrated probes to measure pocket depth and determine periodontal pocket configuration. There have been several generations of probes developed with improvements in standardization, precision, and automation. First generation probes were manual and included the Williams probe. Second generation probes aimed to standardize pressure, like the TPS probe. Third generation probes were automated, like the Florida Probe. Fourth generation probes utilized 3D technology while fifth generation probes combine ultrasound for more accurate measurement without pocket penetration. Studies show electronic probes provide more reproducible measurements than manual probes, though manual probes can have good reproducibility as well depending on the examiner.













































![Advanced_Diagnostic_Aids[1]-1.pdf periodontics](https://cdn.slidesharecdn.com/ss_thumbnails/advanceddiagnosticaids1-1-251217191016-ed832b73-thumbnail.jpg?width=640&height=640&fit=bounds)





















