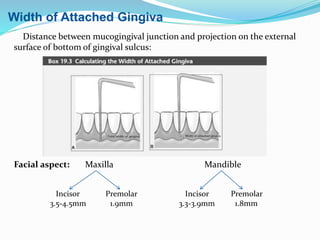
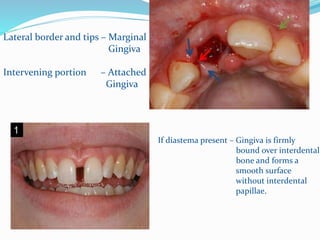
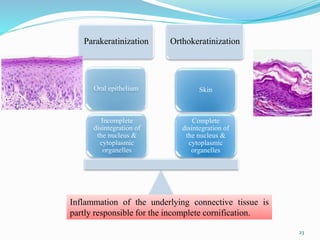
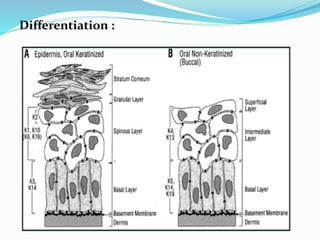
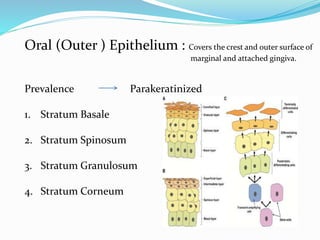
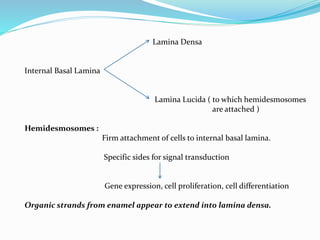
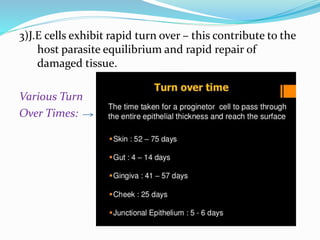
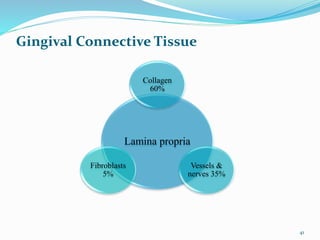
The document provides an overview of the anatomy and histology of the gingiva. It discusses the different layers of the gingiva including the marginal gingiva, attached gingiva, and interdental gingiva. Microscopically, it describes the epithelial layers covering the gingiva and the underlying connective tissue layer. Key points include that the gingival epithelium can be parakeratinized, orthokeratinized, or non-keratinized depending on its location. The junctional epithelium attaches to the tooth surface and renews rapidly. The connective tissue layer mainly comprises collagen fibers, vessels, and fibroblasts. Gingival fluid maintains tissue health and possesses antimicrobial properties