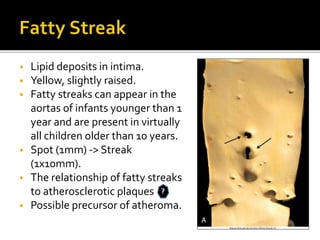
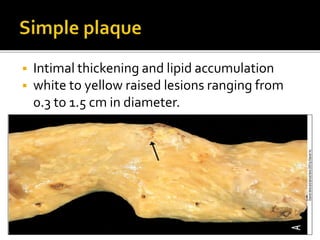
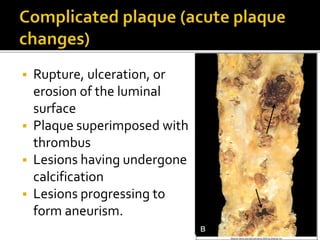
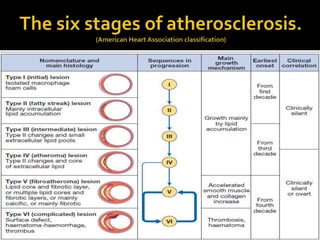
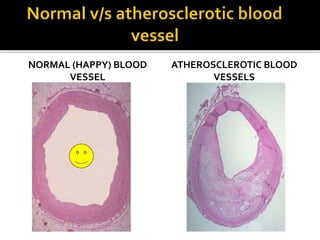
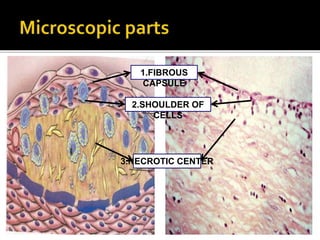
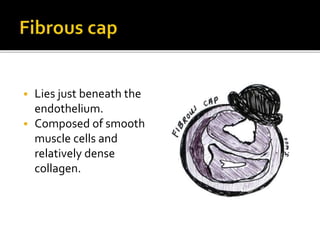
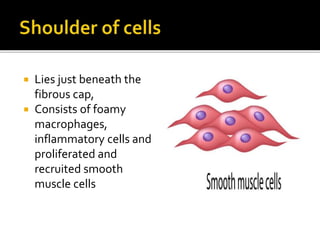
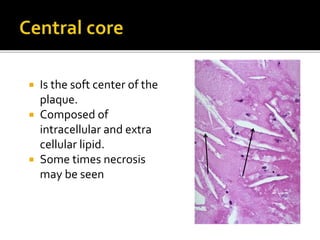
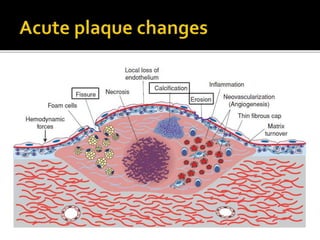
The document discusses the morphology and distribution of atherosclerotic plaques, emphasizing the prevalence of fatty streaks in infants and children. It outlines the stages of plaque progression from fatty streak to complicated plaque, detailing the composition and structure of plaques. The atherosclerotic vessel structure includes a fibrous cap, a shoulder of cells, and a necrotic core, with potential complications such as rupture and aneurysm formation.