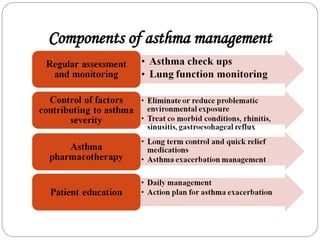
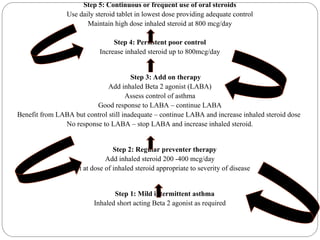
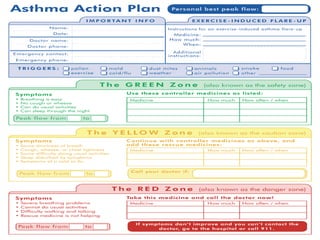
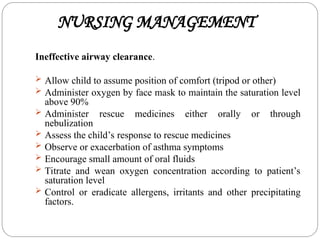
Bronchial asthma is a chronic condition characterized by airway inflammation and reversible obstruction, commonly manifesting in children under four years old. The document outlines the etiology, classification, symptoms, diagnostic evaluations, and management strategies for asthma, emphasizing the importance of recognizing triggers and maintaining proper communication with patients and families. Effective asthma management involves a combination of medication, lifestyle adjustments, and education on managing triggers and responding to exacerbations.

















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
