



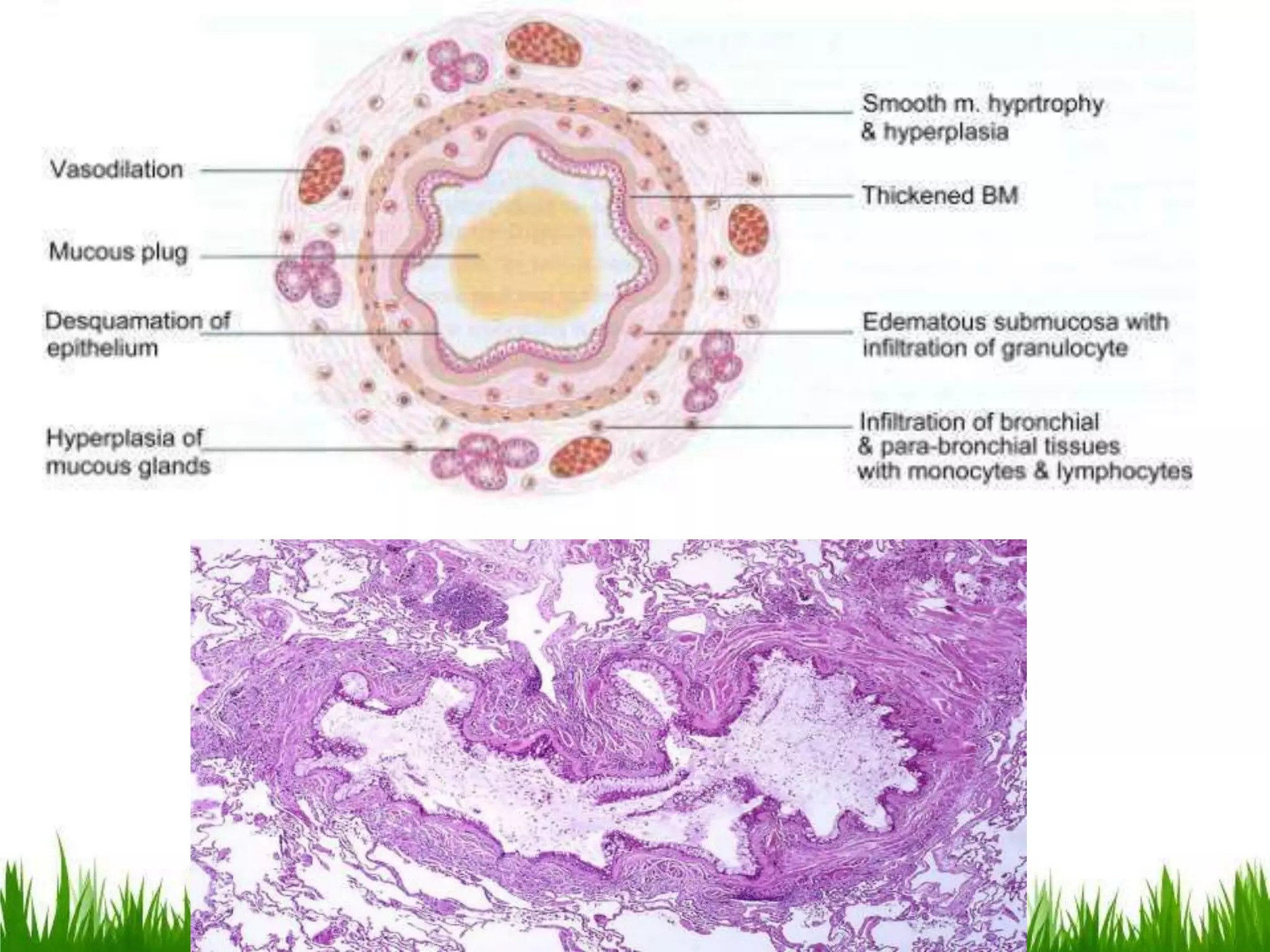





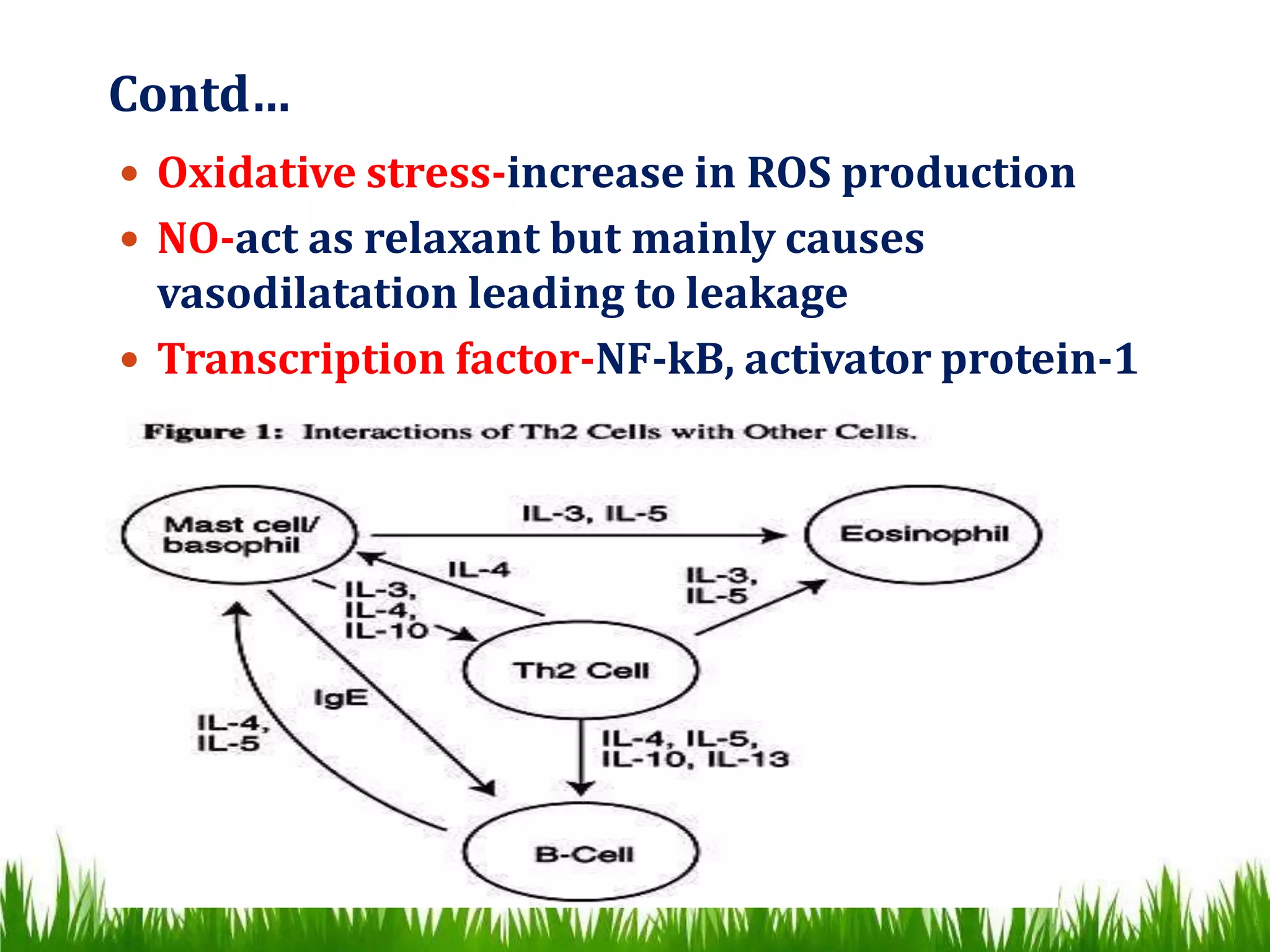




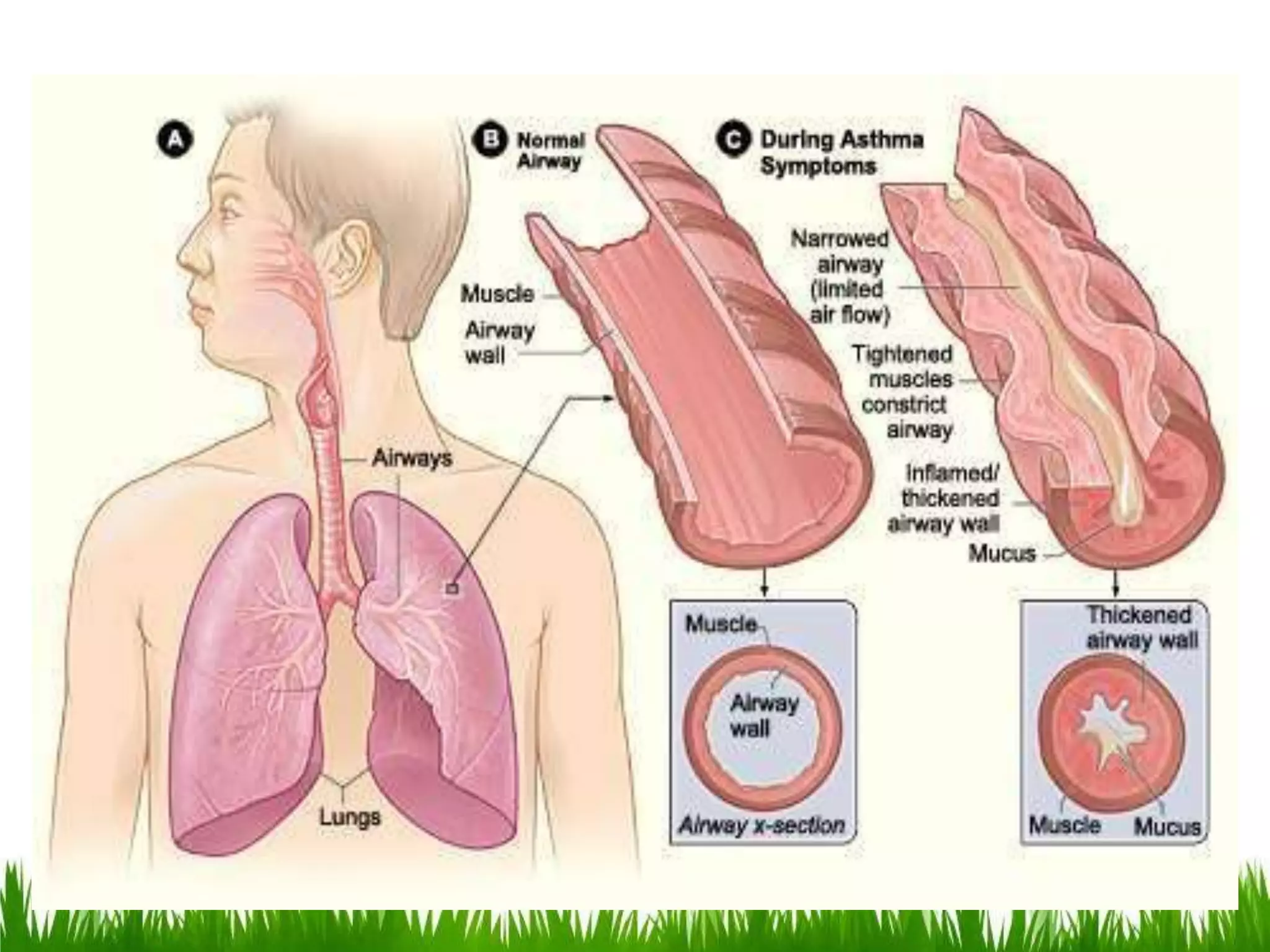
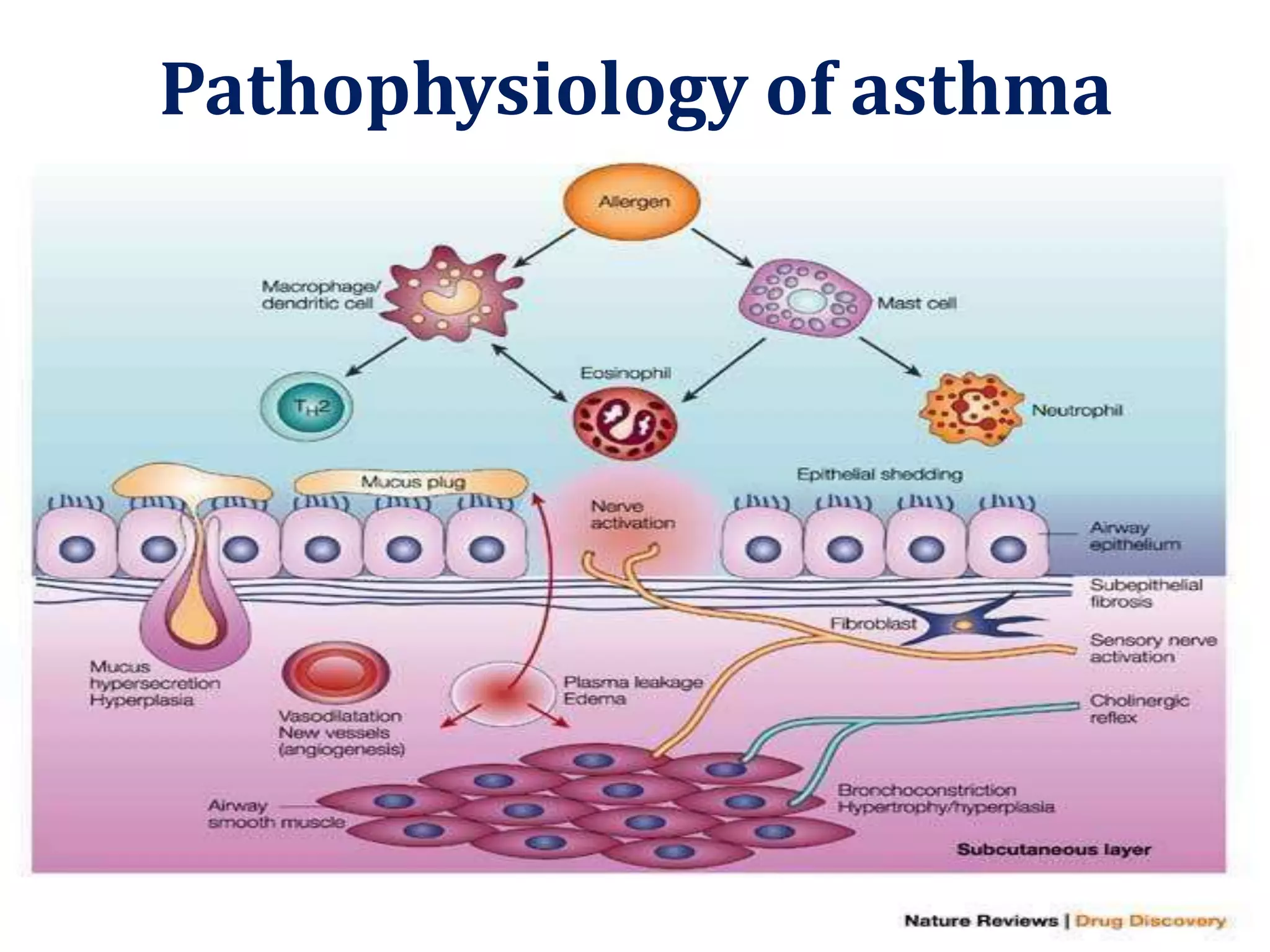




Asthma is a chronic inflammatory disorder characterized by variable airflow obstruction. It involves eosinophilic infiltration and thickening of the basement membrane, as well as hyperplasia of glands and vasodilatation. IgE-dependent mast cell activation releases various inflammatory mediators, causing early and late phase reactions involving dendritic cells and TH2 cells. This leads to epithelium shedding, fibrosis, smooth muscle hypertrophy, and increased permeability. Long-term inflammation can also cause airway remodeling.