Downloaded 274 times
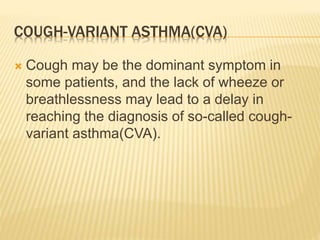
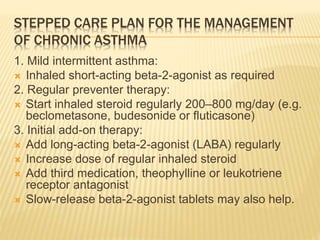
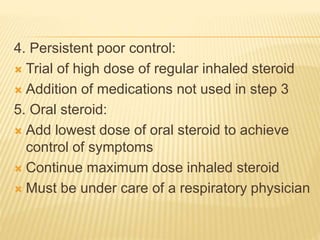
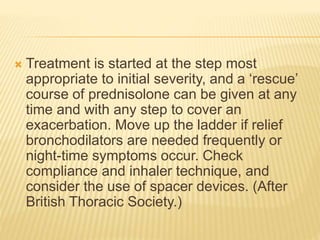
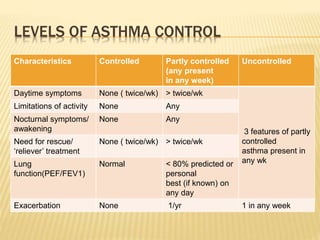
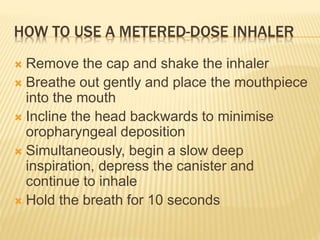
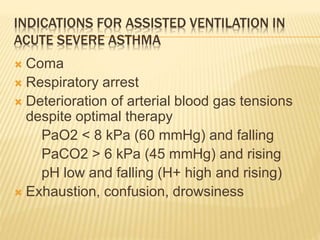
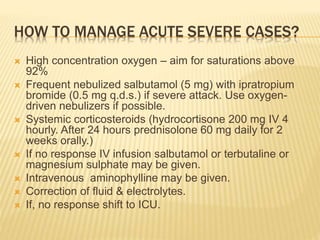
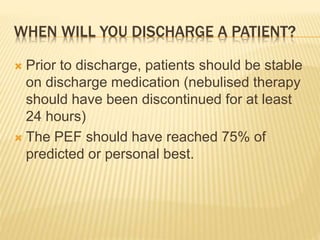
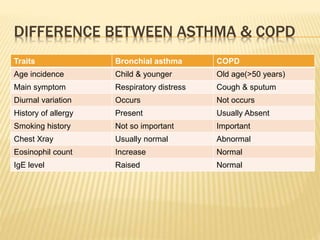

This document provides an overview of bronchial asthma, including its definition, pathophysiology, types, triggers, symptoms, diagnosis, management, and differences from COPD. Key points include: - Asthma is a disease characterized by reversible airway obstruction and inflammation in response to various stimuli. It is an IgE-mediated hypersensitivity reaction. - Common symptoms include wheezing, chest tightness, cough and breathlessness. Diagnosis is based on clinical history and pulmonary function tests showing improved airflow with bronchodilators. - Management involves avoidance of triggers, bronchodilators, inhaled corticosteroids, and a stepped treatment plan escalating medications based on asthma control. Acute































































![Microsoft PowerPoint - Asthma 4th year Lecture (1) [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-220716165932-01cf3f8c-thumbnail.jpg?width=640&height=640&fit=bounds)


![Microsoft+PowerPoint+-+Asthma+4th+year+Lecture+(1)+[Compatibility+Mode].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/microsoftpowerpoint-asthma4thyearlecture1compatibilitymode-230704125445-487a63ed-thumbnail.jpg?width=640&height=640&fit=bounds)














![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







