Downloaded 74 times







![REFERENCES
• Baker PN, Kenny LC(eds). Obstetrics by Ten Teachers. 19th ed. London: Hodder
Arnold; 2011.
• Collins S, Arulkumaran S, Hayes K, Jackson S, Impey L. Oxford Handbook of
Obstetrics and Gynaecology. 3rd ed. Collins S, Arulkumaran S, Hayes K, editors.
United Kingdom: Oxford University Press; 2013.
• Medscape: Forceps Delivery [online]. 11th December 2013. Extracted on 17th April
2015.
Available at: http://emedicine.medscape.com/article/263603-overview#a05
• Healthline: Types of Forceps Used in Delivery [online]. 15th March 2012.
Extracted on 17th April 2015.
Available at: http://www.healthline.com/health/pregnancy/assisted-delivery-types-
forceps#TypesofForceps1
• Brookside Associates: Obstetric and Newborn Care [online]. 2007. extracted on
17th April 2015.
Available at:
http://www.brooksidepress.org/Products/Obstetric_and_Newborn_Care_II/lesson_5_Section_1.htm](https://image.slidesharecdn.com/assisteddeliveries-151124152107-lva1-app6892/85/Assisted-deliveries-13-320.jpg)

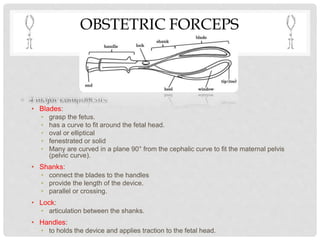
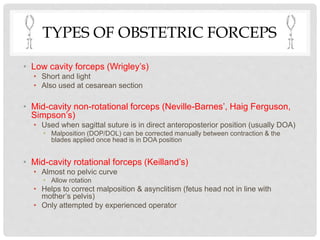
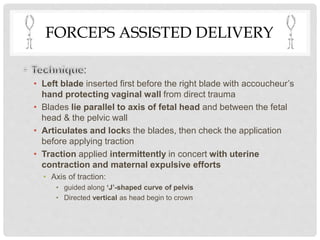
This document describes forceps-assisted deliveries. It defines obstetric forceps as a double-bladed metal instrument used to extract the fetal head. It describes the parts of forceps including the blades, shanks, locks and handles. It discusses different types of forceps and their uses. It outlines the indications, prerequisites, technique and contraindications for a forceps-assisted delivery. Key steps include inserting the blades one at a time, applying traction in line with uterine contractions to deliver the baby. Training and experience of the operator are important to minimize risks.





























































































