Downloaded 194 times

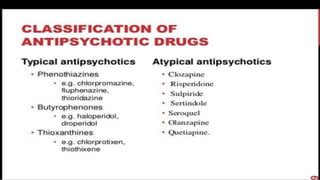
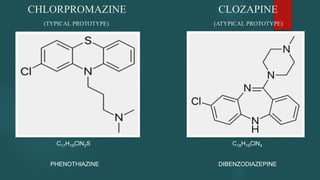
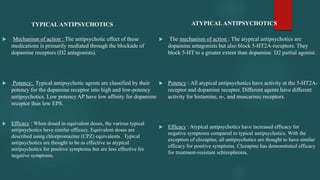
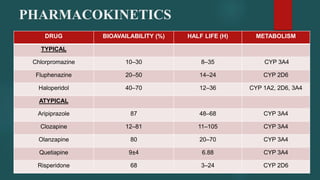
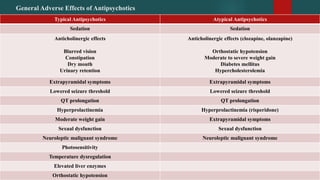

This document summarizes key differences between typical and atypical antipsychotics. It discusses their mechanisms of action, efficacy, side effect profiles, pharmacokinetics, and drug interactions. Typical antipsychotics work mainly through D2 receptor antagonism and have higher rates of extrapyramidal side effects, while atypicals have additional 5-HT2A antagonism and generally cause more metabolic side effects like weight gain. Both classes present risks like QT prolongation, NMS, and low seizure thresholds that require monitoring.







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





