Downloaded 22 times

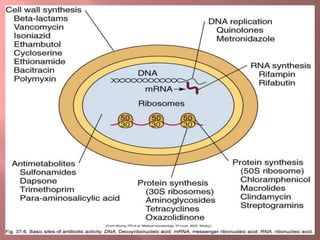

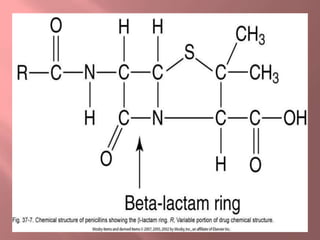






This document discusses various classes of antibiotics including penicillins, cephalosporins, macrolides, tetracyclines, aminoglycosides, and quinolones. It describes their mechanisms of action, common uses, and potential adverse effects. Specifically, it provides details on common drugs in each class, how they work at the cellular level to kill bacteria, infections they can treat, and side effects to monitor like ototoxicity and nephrotoxicity. The document stresses the importance of obtaining cultures before treatment and monitoring patients for both therapeutic responses and unwanted reactions.