Downloaded 414 times


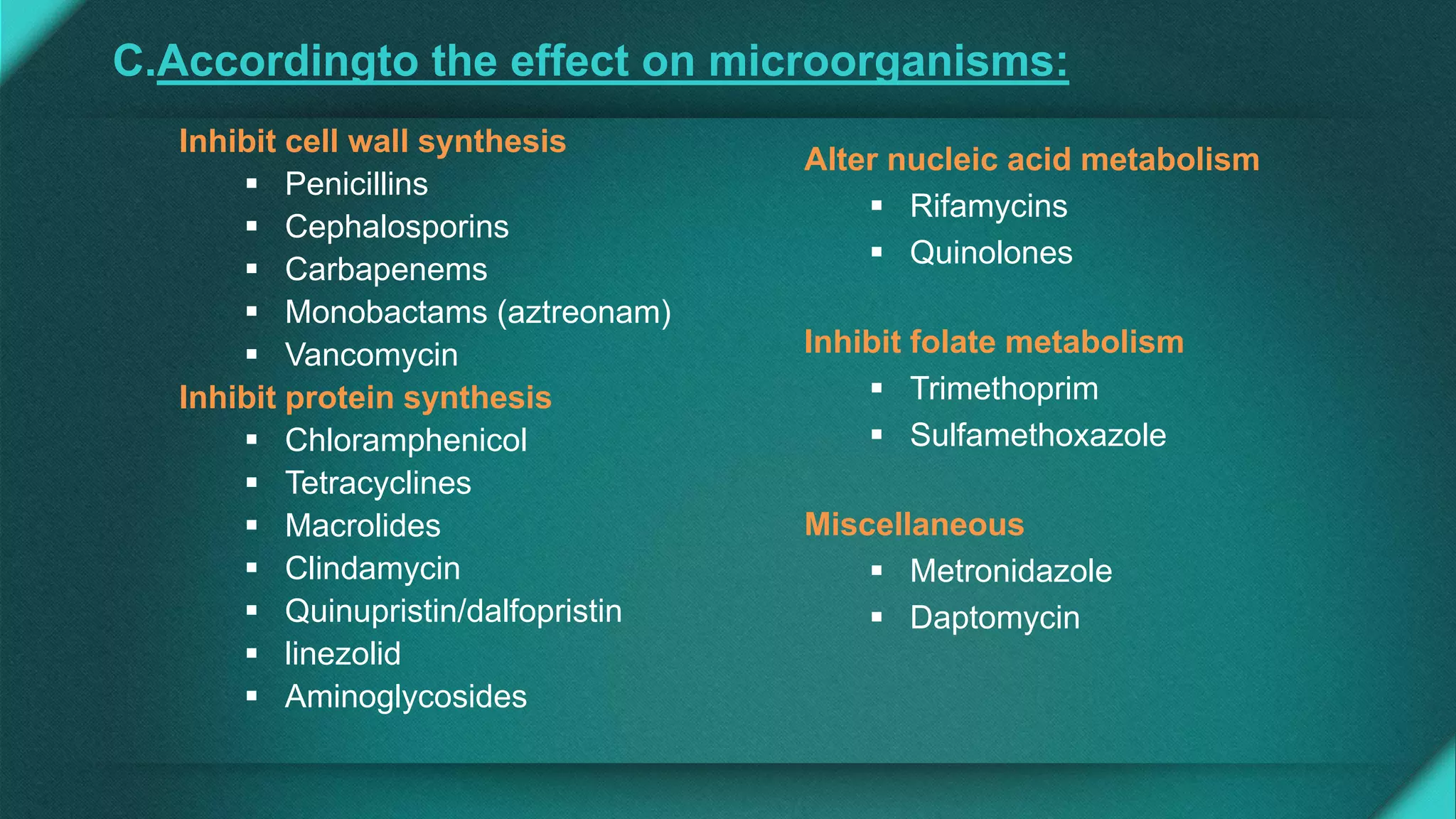
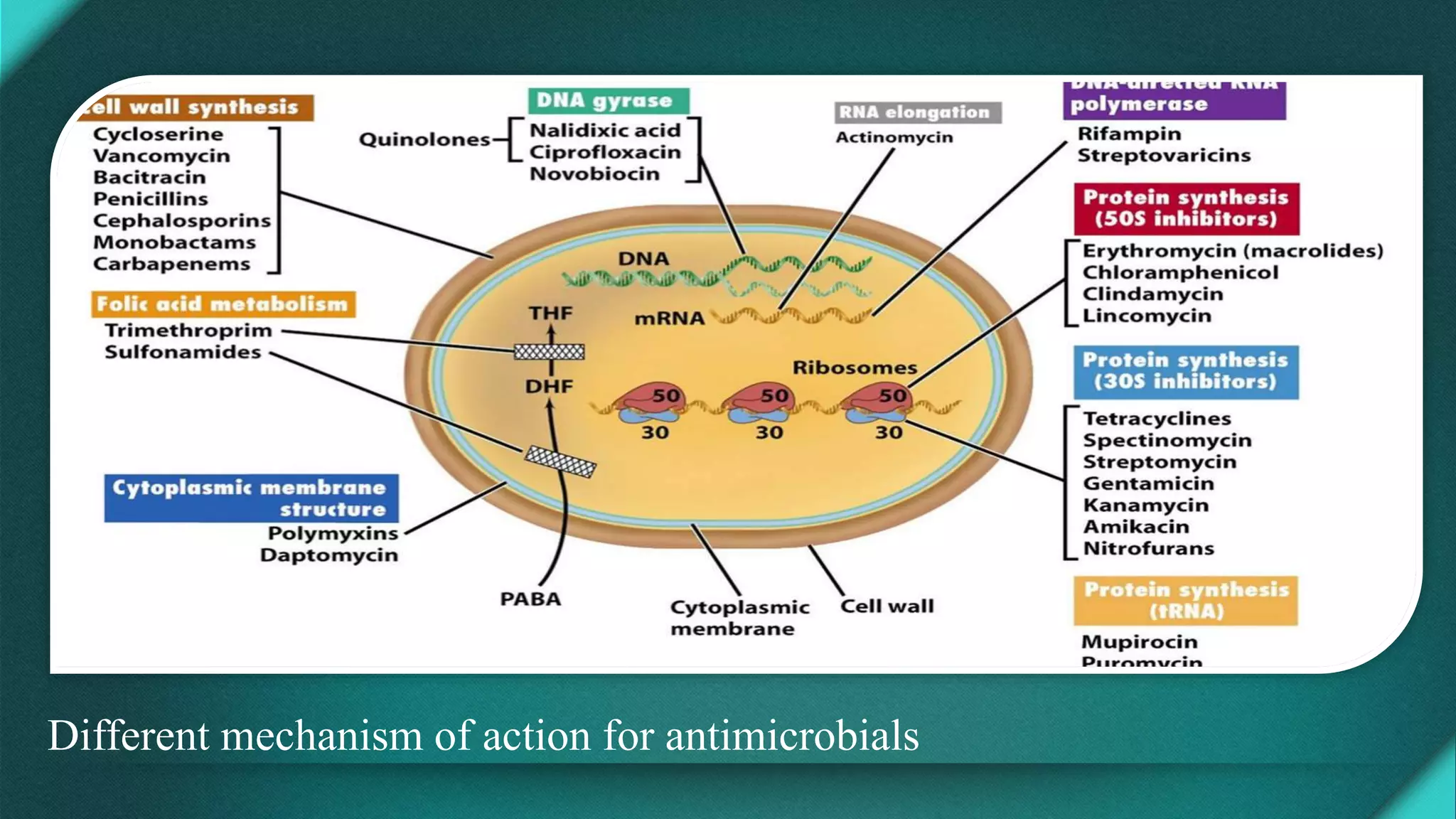
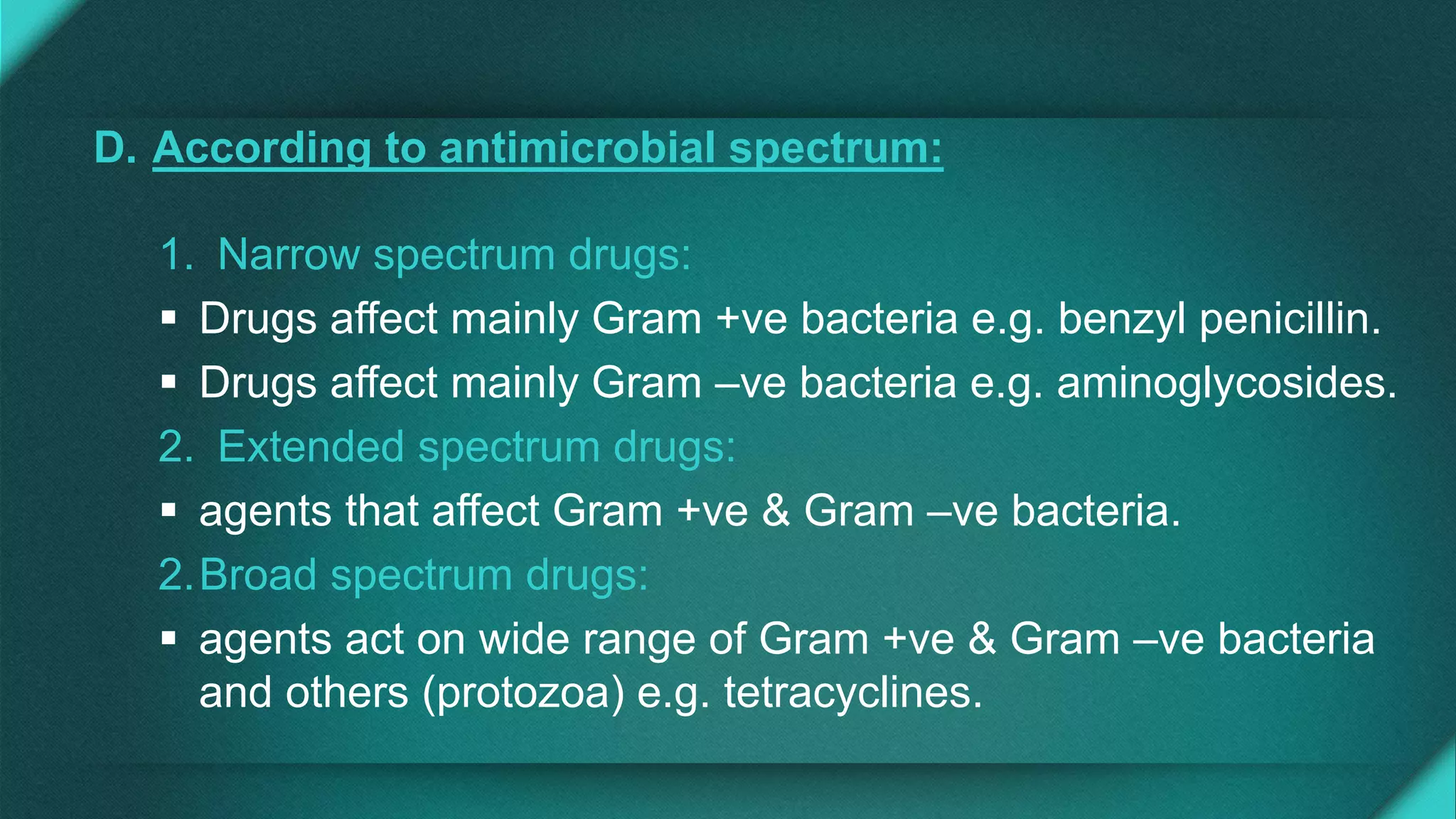
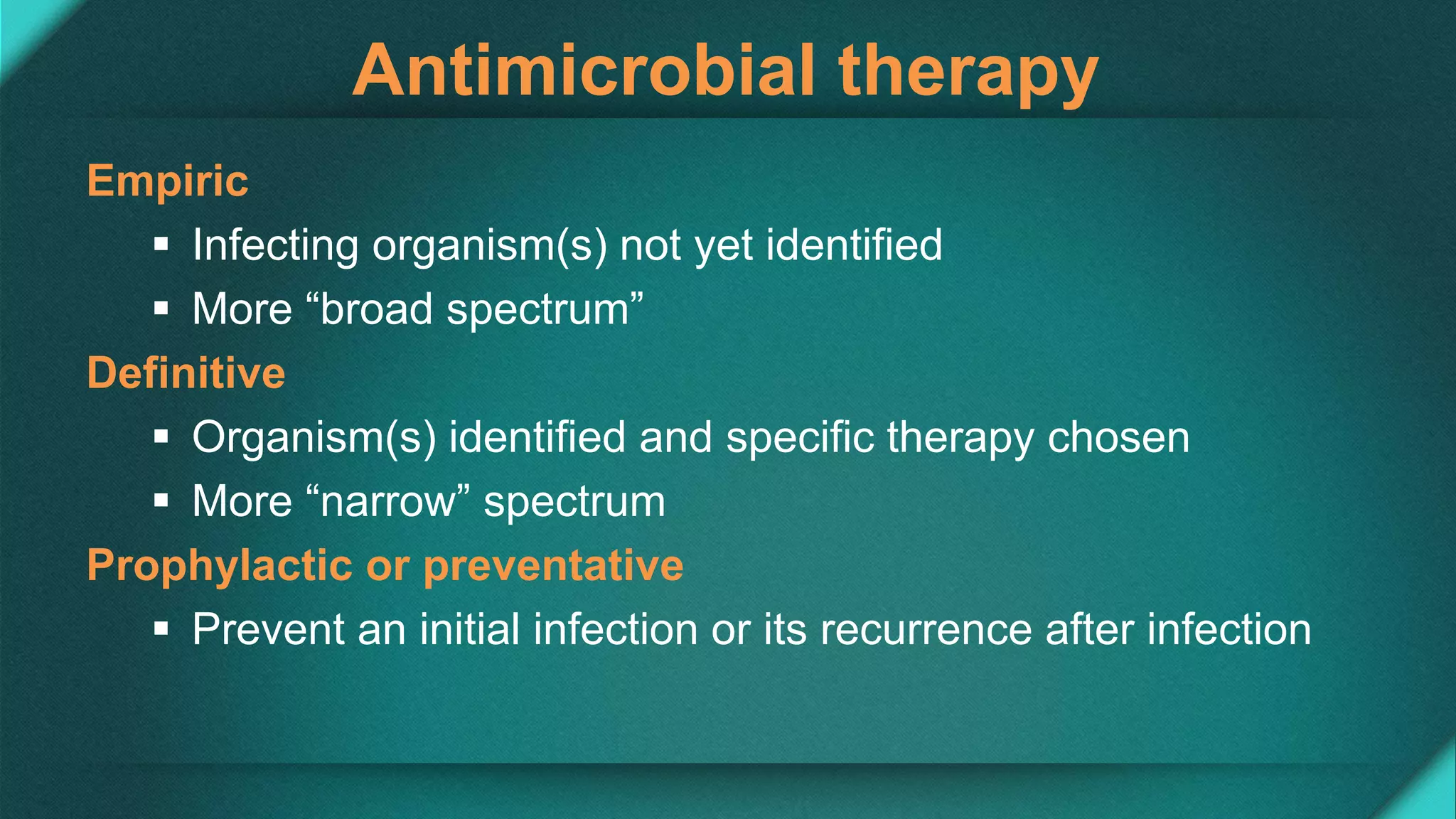


















This document discusses principles of antimicrobial therapy. It begins by classifying antimicrobials based on their source, mechanism of action, spectrum, and effect on microorganisms. Different mechanisms of action for various classes of antimicrobials are described. A clinical approach for rational prescribing is then outlined, including confirming the presence of an infection, selecting agents based on patient factors and tissue penetration, and determining dosing based on pharmacodynamics. Monitoring efficacy and toxicity is also discussed. Adverse effects like hypersensitivity, superinfection, and antibiotic resistance are reviewed.









































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)













