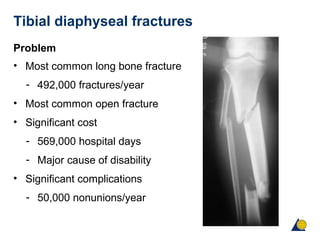
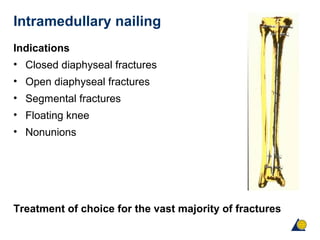
This document discusses the treatment of closed tibial shaft fractures. It notes that tibial fractures are common and can lead to complications if not treated properly. Treatment options include nonoperative care with casting or operative fixation with intramedullary nails, plates, or external fixators. The choice of implant depends on factors like the fracture pattern and soft tissue injury. Intramedullary nailing is often the treatment of choice as it allows indirect reduction and preserves soft tissues. Surgical technique and avoiding complications like compartment syndrome are also discussed.










![Reamed or unreamed nails?
Closed tibial fractures [CM Court-Brown et al 1996]
Reamed nails
• Union (weeks) 15.4
• Nonunion 0%
• Malunion 0%
• Screw breakage 4%
• Nail breakage 0%
Unreamed nails
• Union (wks) 22.8
• Nonunion 20%
• Malunion 16%
• Screw breakage 52%
• Nail breakage 4%
Reamed mechanically and biologically superior.](https://image.slidesharecdn.com/ueholyb9qymqzjw0dvma-signature-adb10c2637e590b7c6a491acd596fa5528ae126ffab840d71ae72dd1362a57b8-poli-160422234113/85/Closed-tibial-shaft-28-320.jpg)