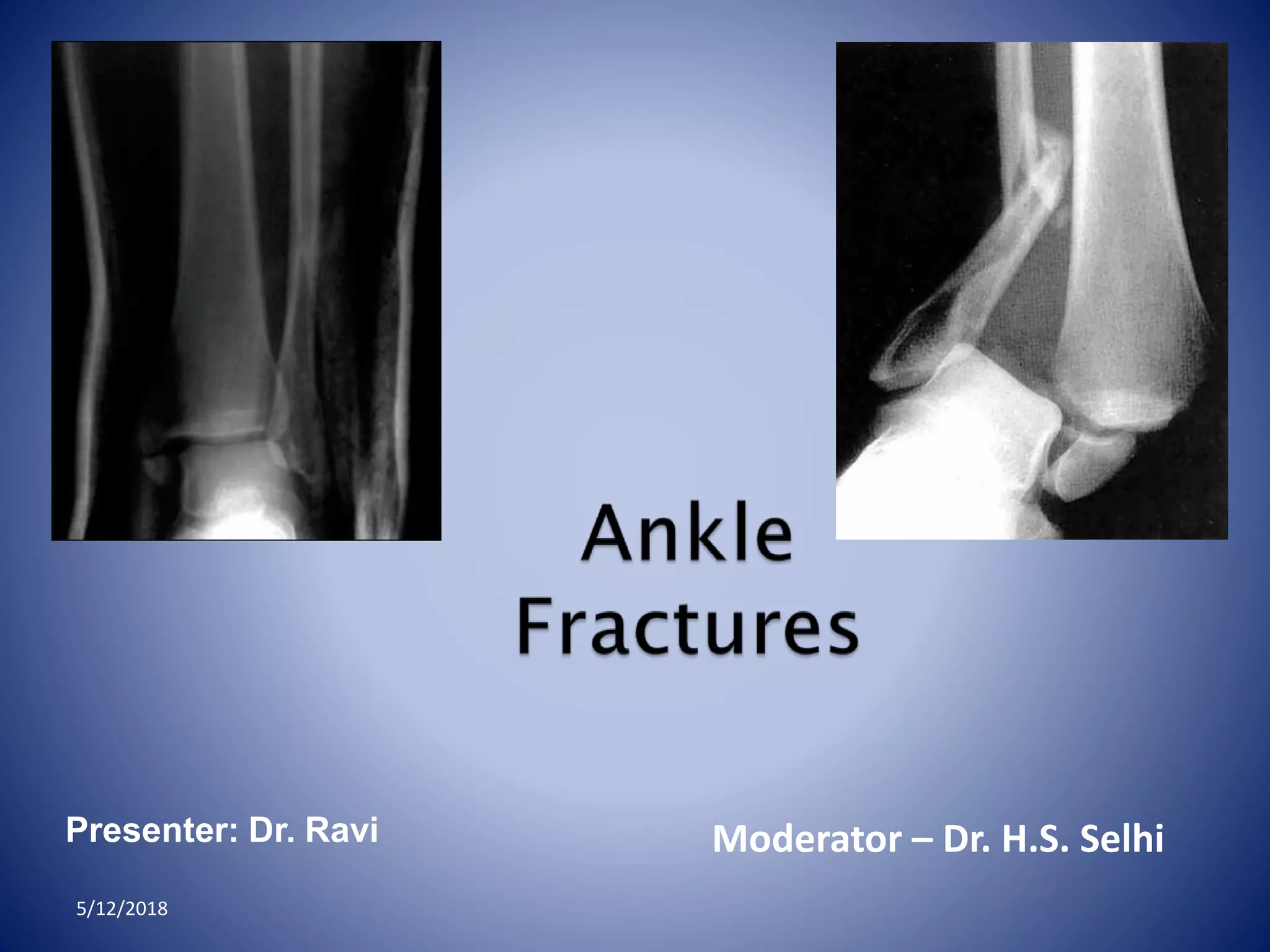
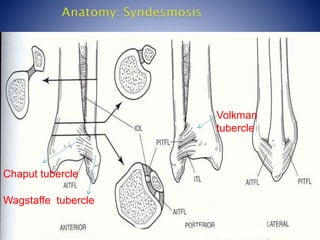
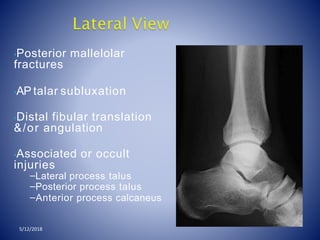
Ankle fractures are common injuries, accounting for 10% of all fractures. The ankle is a three bone joint composed of the tibia, fibula, and talus. Stability of the ankle depends on intact medial and lateral ligament complexes. Classification systems help describe the pattern and severity of the injury. Treatment depends on restoring anatomy and stability through closed or open reduction and fixation.





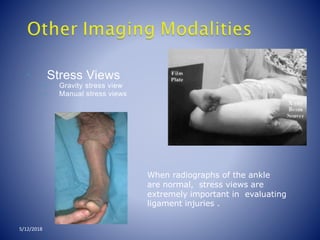


![GOAL: TO EVALUATE DEEP DELTOID [i.e.
INSTABILITY]
Medial tenderness,
swelling, echymosis
STRESS VIEWS- GRAVITY OR
MANUAL
5/12/2018](https://image.slidesharecdn.com/anklefracturesfinal-180512105501/85/Ankle-fractures-final-45-320.jpg)































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






