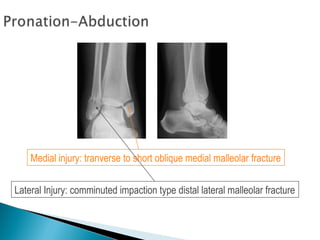
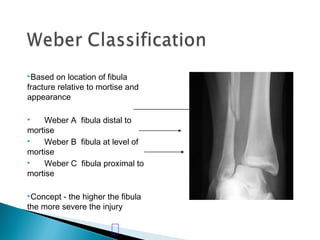
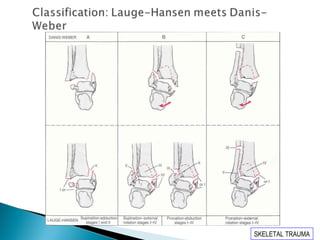
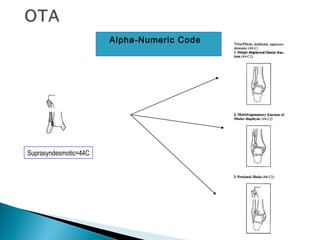
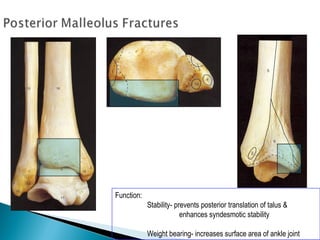
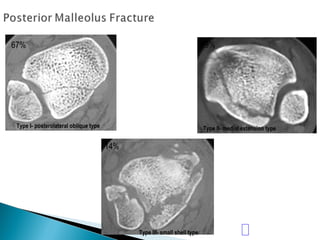
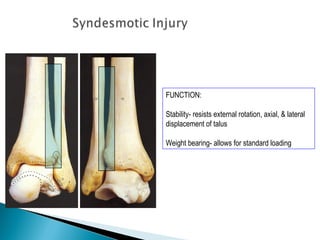
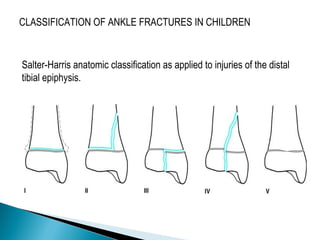
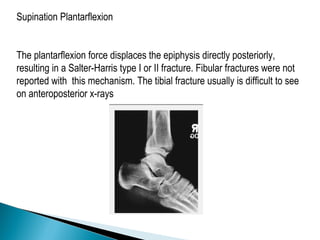
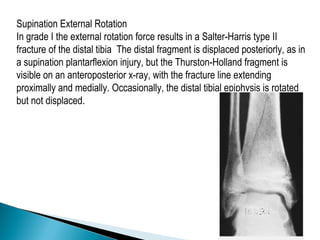
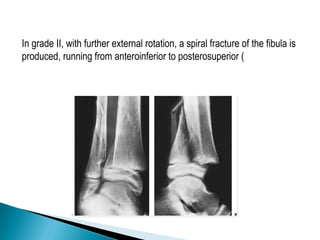
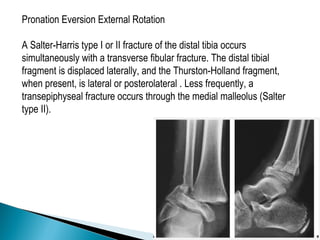
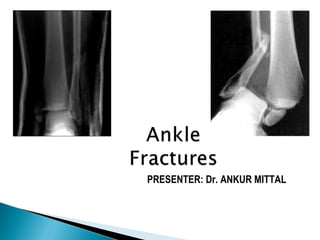
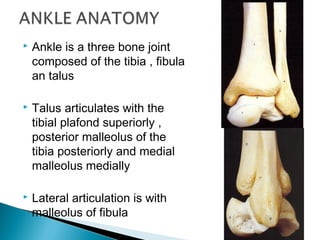
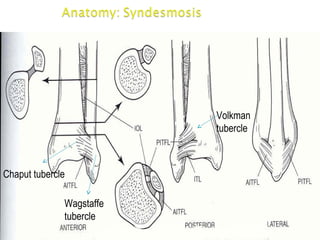
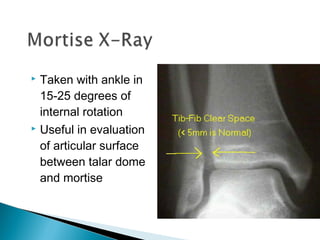
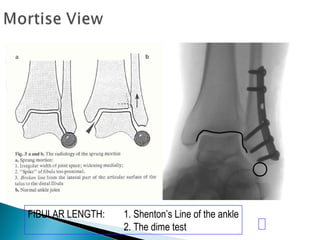
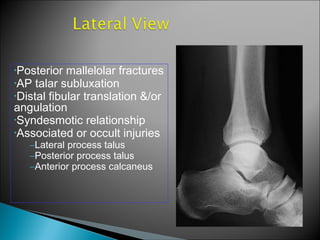
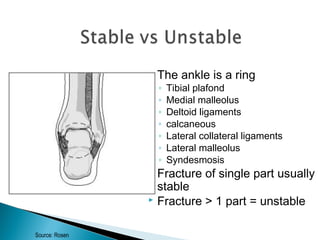
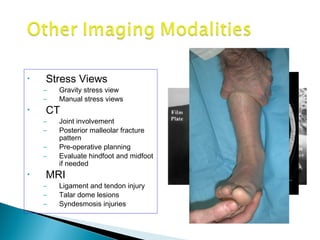
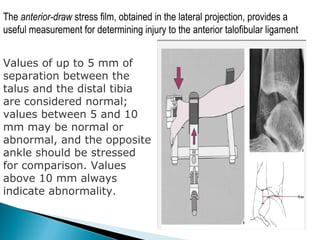
The ankle is a three bone joint composed of the tibia, fibula, and talus. The talus articulates superiorly with the tibial plafond and posteriorly with the posterior malleolus of the tibia. Laterally, it articulates with the fibula. Ankle fractures are commonly evaluated using plain films of the ankle in AP, mortise, and lateral views. Stress views may also be used to evaluate ligament injuries. Classification systems like Lauge-Hansen describe the mechanism of injury and associated soft tissue damage. Accurate reduction and restoration of the ankle mortise is important for surgical treatment of unstable ankle fractures.


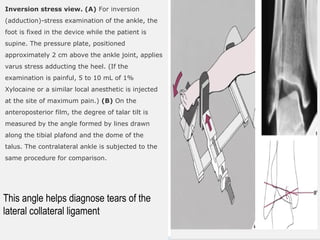

![GOAL: TO EVALUATE DEEP DELTOID [i.e. INSTABILITY]
METHOD: MEDIAL TENDERNESS
MEDIAL SWELLING
MEDIAL ECCHYMOSIS
STRESS VIEWS- GRAVITY OR MANUAL](https://image.slidesharecdn.com/anklefracturesfinal-120314092959-phpapp01-150806181221-lva1-app6892/85/Anklefracturesfinal-120314092959-phpapp01-44-320.jpg)