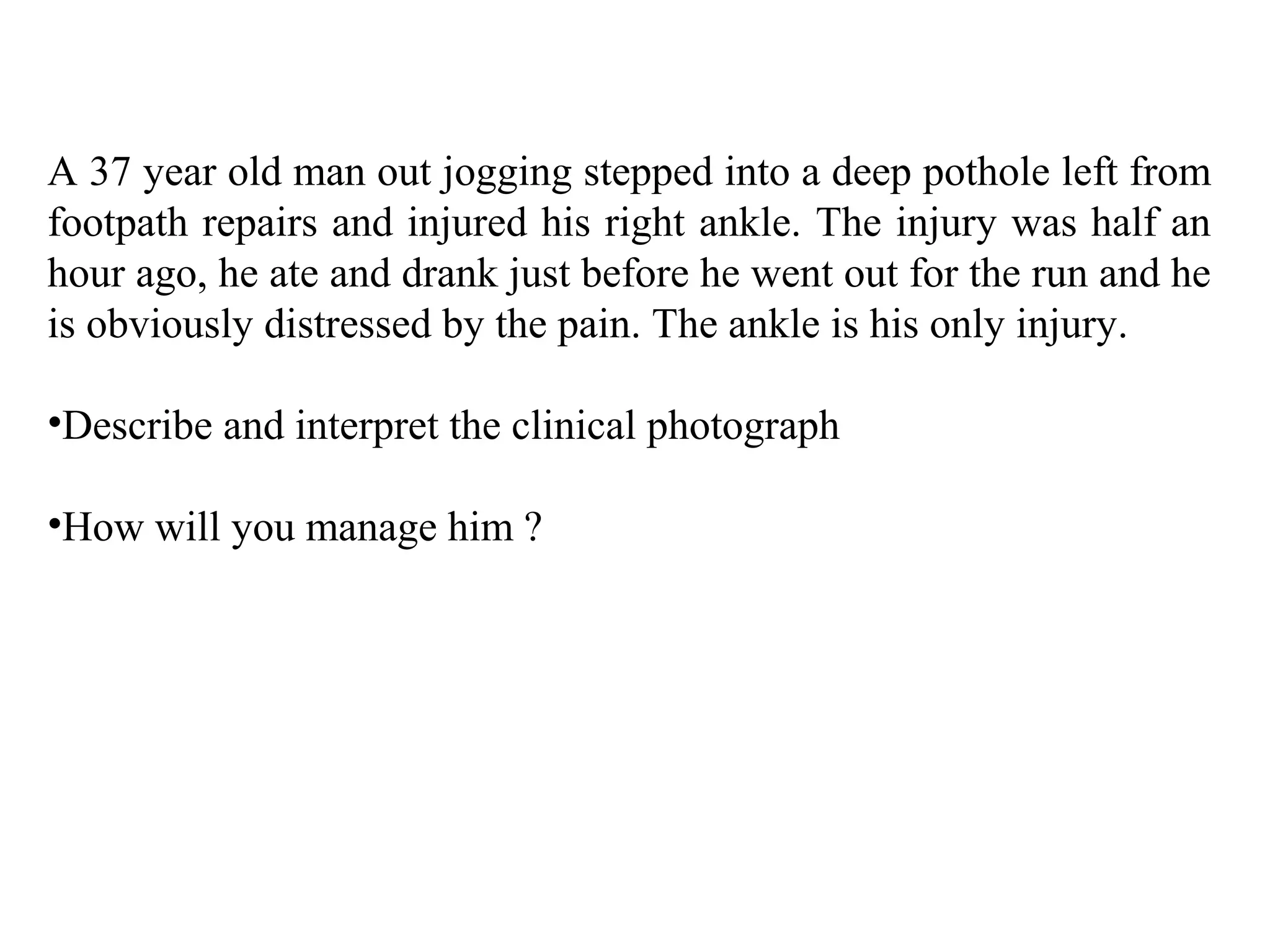
A 37-year old man injured his right ankle after stepping in a pothole while jogging. His ankle appears deformed with the foot displaced laterally and posteriorly. The skin over the lower tibia also appears stretched and pale. This clinical presentation is most consistent with a fracture dislocation at the ankle joint. The priorities are to provide analgesia, reduce the injury in the emergency department to preserve skin integrity, and obtain an x-ray for orthopedic guidance before definitive repair. Initial analgesia could include nitrous oxide and narcotics, with additional sedation like propofol or ketamine if needed despite his fasting status.