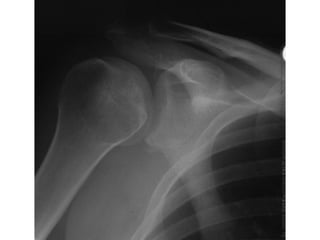
The x-ray shows a posterior dislocation of the footballer's right shoulder. Key signs on the x-ray include a symmetrical "light bulb" shaped humeral head and widening of the gleno-humeral joint space. There is also likely a fracture fragment at the inferior rim of the glenoid. The injury should be managed by reducing the dislocation under procedural sedation using traction, abduction, and external rotation, known as the Milch method.