Angina pectoris is caused by reduced oxygen supply to the heart muscle due to spasm or obstruction of the coronary arteries. There are three main types of angina - stable angina, variant angina, and unstable angina. The main causes are atherosclerosis and coronary artery spasm. Treatment goals are to reduce symptoms and mortality from coronary artery disease progression through lifestyle changes, drug therapy, and surgical methods when needed. Drug therapy includes nitrates, calcium channel blockers, beta blockers, and other vasodilators to relieve symptoms and reduce ischemia. Percutaneous coronary intervention and coronary artery bypass grafting are surgical options for severe cases.
ANGINA PECTORIS –ETIOLOGY AND
TREATMENT
Shreya Bhattacharjee
B.Pharm. Semester VI
Class Roll No. B14014
2.
ACKNOWLEDGEMENT
I would liketo express my special thanks of gratitude to Mr. Mrittunjoy
Mojumdar sir, to Mr. Suman Adhikari sir as well as our principal Dr. Arnab
Samanta sir who gave me the golden opportunity to do this wonderful project
on the topic Angina Pectoris – etiology and treatment, which also helped me in
doing a lot of research and I came to know about so many new things. I am
really thankful to them for helping me throughout this project.
I would also like to thank other teachers and my parents who helped me a lot
in finalizing the project within the limited time frame.
TYPES
STABLE ANGINA /
CLASSICANGINA
VARIANT ANGINA /
PRINZMETAL ANGINA
UNSTABLE ANGINA /
CRESCENDO
ANGINA
Atherosclerosis Coronary Spasm Atherosclerosis with
blood clot
Occurs with exertion or
exercise
Severe pain often occurs
at rest or minimal
exertion
Typically at rest during
night or early morning
hours
Relieved by rest or
antianginals
Relieved by anti -
angina drugs
(Nitroglycerin)
Not relieved by rest
or medication
5
2
1.Choking, smothering, squeezing,or crushing pressure in the centre of
chest.
2. Patients with atherosclerosis also may experience sweating,
clamminess.
3. Shortness of breath (dyspnea).
1.Angina pain may radiate to the shoulders, arms, back, neck, or
jaw.
2. The pain may be of any intensity from mild to severe.
Angina itself is a symptom (or a set of symptoms) of Ischemic heart disease
(IHD) , not a disease.
CLINICAL PRESENTATION
8
5
9.
Stable angina occurswith a certain amount of stress or physical
activity. Occurs for a shorter time and does not cause more often.
Unstable angina is sudden, more severe and more frequent.
* Pain increases every time.
* Lasts longer than 15-20 minutes.
* Does not respond well even under medication.
* Requires immediate attention.
CLINICAL PRESENTATION (contd.)
9
6
GOALS OF TREATMENT
Alltreatments for people with coronary artery disease have the
same goals:
- to decrease the effects of the disease on the quality of life and
alleviate symptoms.
- to reduce mortality due to CAD progression.
Above goals can be achieved by following ways:-
* Lifestyle changes
* Drug Therapy
* Surgical methods
11
8
12.
LIFESTYLE CHANGES
•Stress shouldbe reduced.
•Smoking should be stopped.
•There should be sufficient amount of physical exercise and it’s necessary to keep
body weight under control.
•Eat a healthy diet with limited amounts of saturated fat, Trans fat and salt.
12
9
13.
DRUG THERAPY
NITRATES
Denitrated enzymaticallyin smooth
cells to release reactive free radical
nitric oxide (NO).
It activates cytostolic guanyl cyclase.
.
Increases cyclic guanosine mono
phosphate (cGMP) .
It causes dephosphorylation of
myosin light chain kinase (MLCK)
through cGMP dependent protein
kinase.
Reduction in phosphorylated MLCK
interferes with myosin and fails contraction.
Relaxation occurs due to reduced calcium
entry.
a) Short acting
- Nitroglycerin
- glyceryltri nitrate
b) Long acting
- Isosorbide
mononitrate
- Isosorbide
dinitrate
13
10
14.
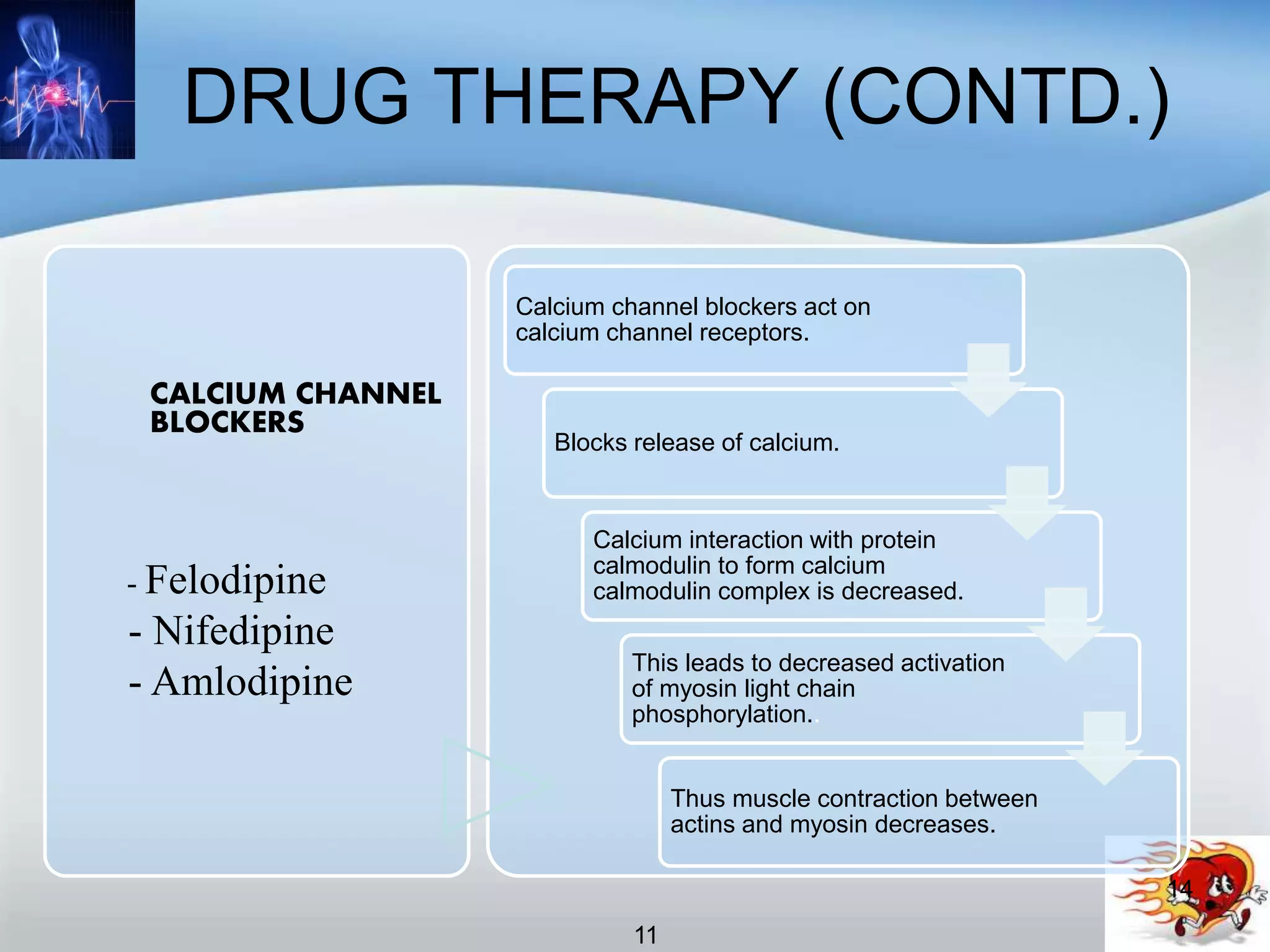
DRUG THERAPY (CONTD.)
CALCIUMCHANNEL
BLOCKERS
- Felodipine
- Nifedipine
- Amlodipine
Calcium channel blockers act on
calcium channel receptors.
Blocks release of calcium.
Calcium interaction with protein
calmodulin to form calcium
calmodulin complex is decreased.
This leads to decreased activation
of myosin light chain
phosphorylation..
Thus muscle contraction between
actins and myosin decreases.
14
11