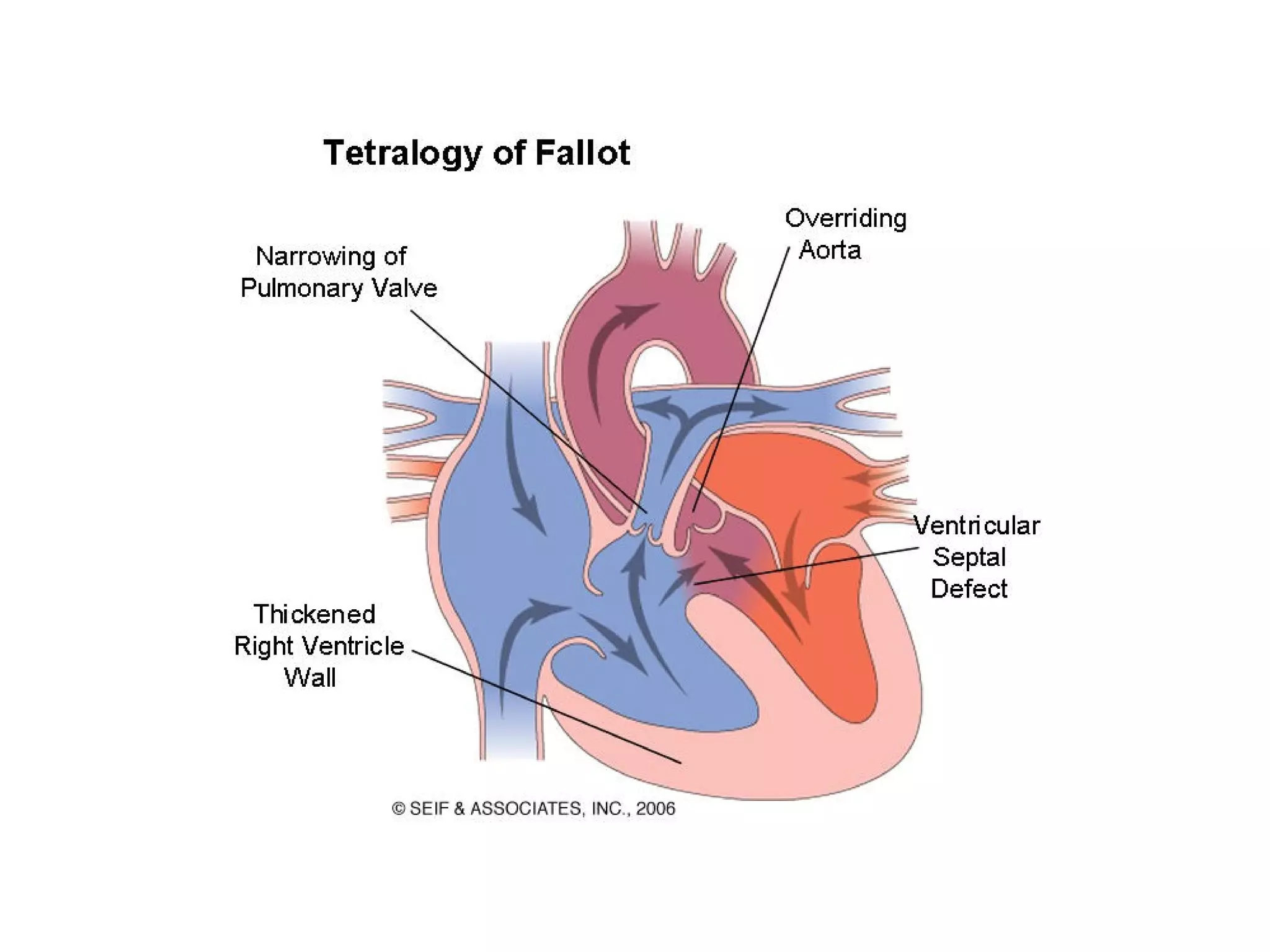
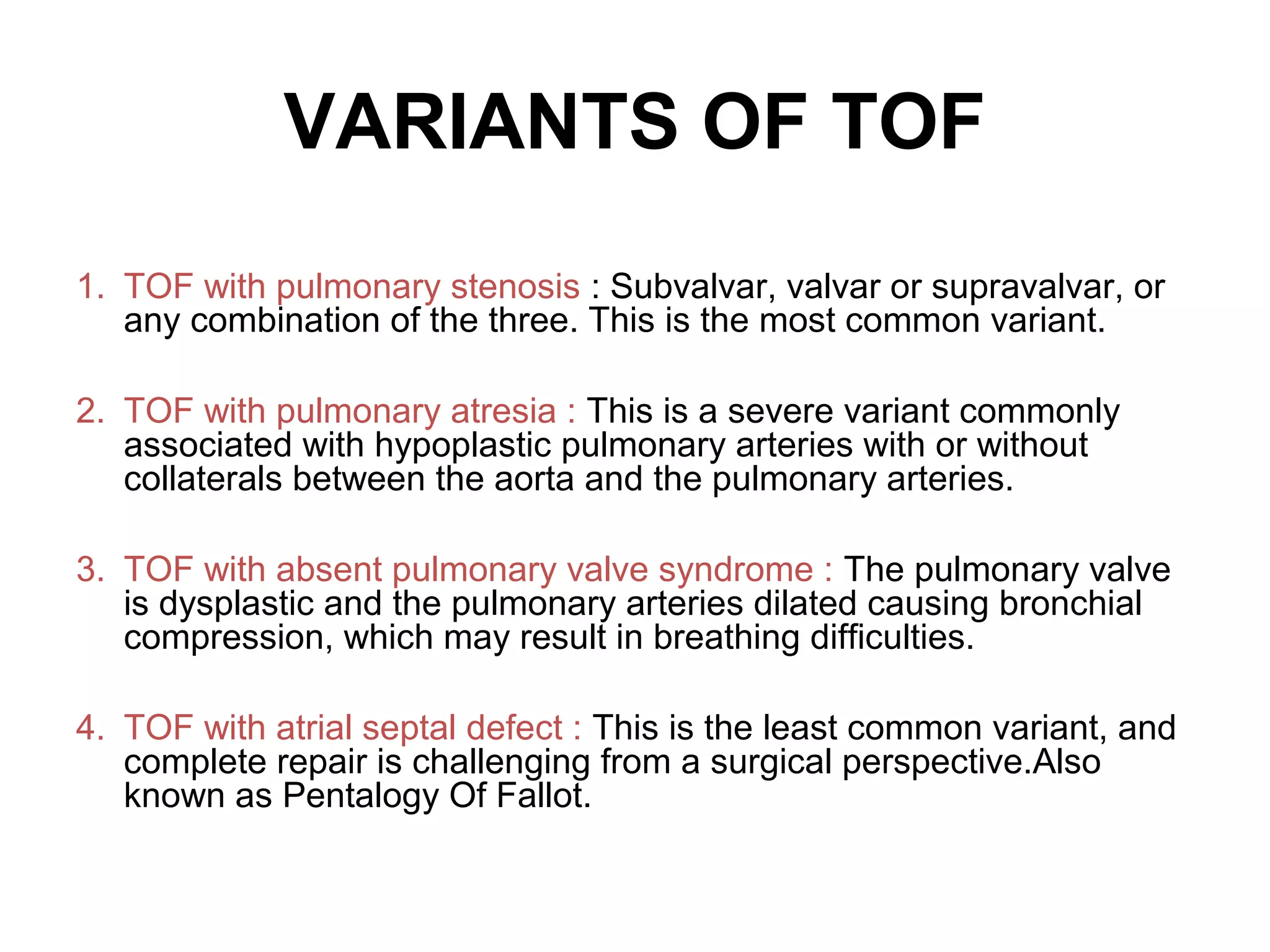
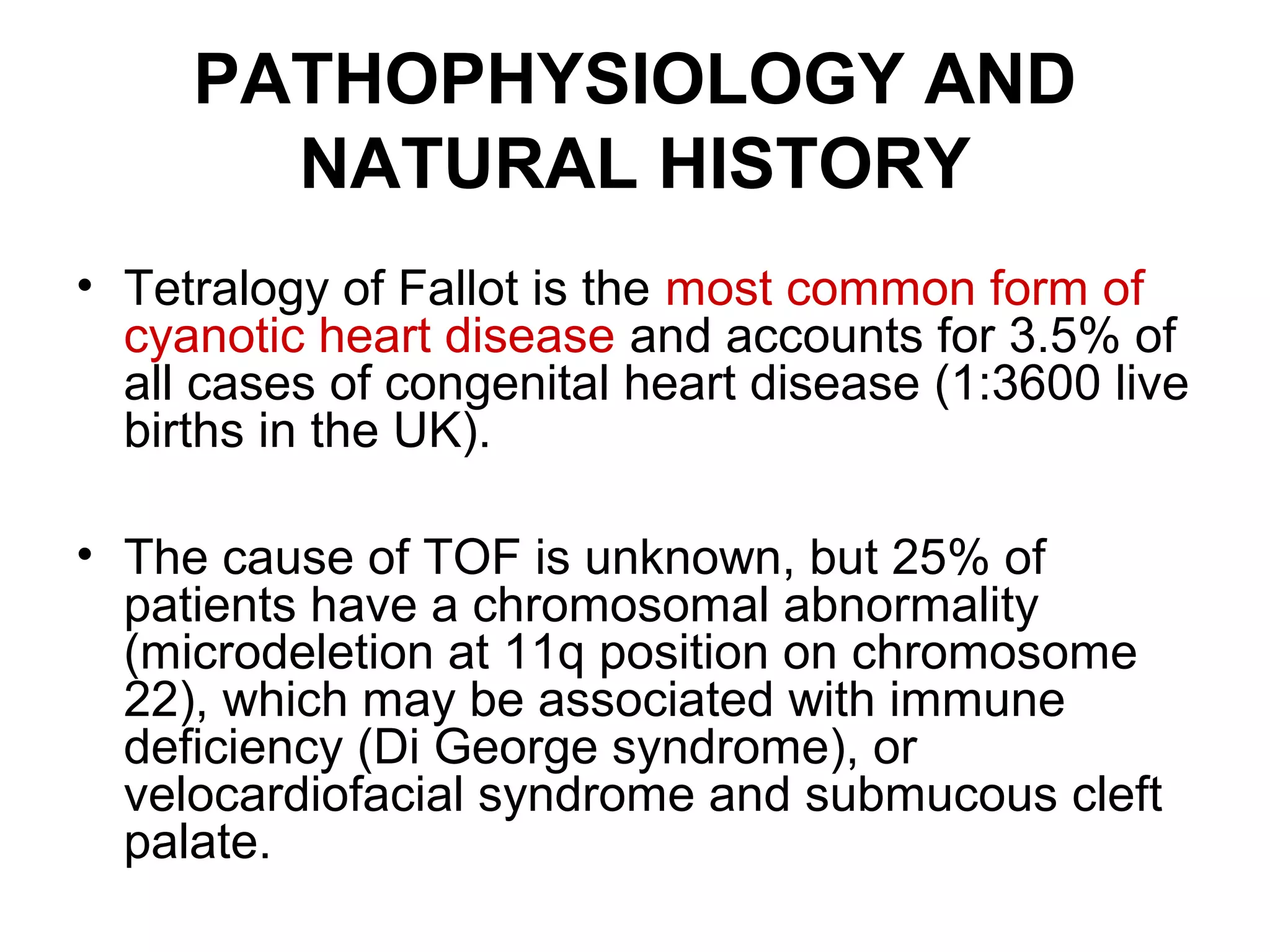
This document provides information on the anaesthetic management of surgery for Tetralogy of Fallot (TOF). It describes the key anatomical features of TOF and its variants. It outlines the natural history of untreated TOF, including risks of cyanotic spells, heart failure and early death. The document discusses the goals of palliative and corrective surgeries, including the modified Blalock-Taussig shunt. It provides guidance on preoperative evaluation, intraoperative management and goals of anaesthesia to optimize hemodynamics and oxygenation during surgery.