Downloaded 276 times
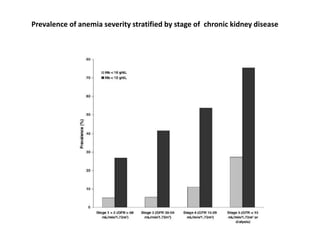

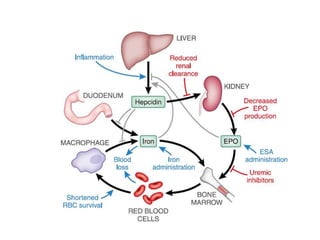
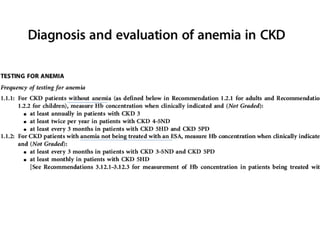
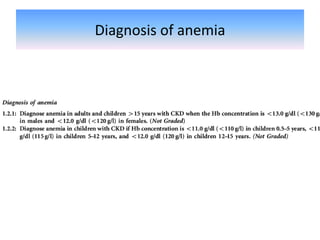
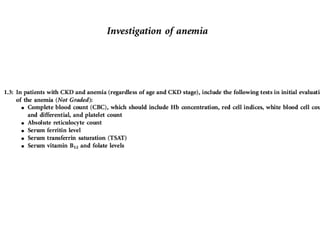
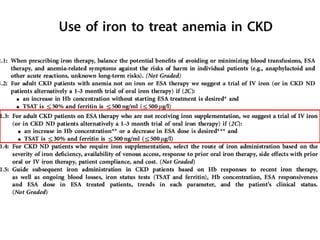
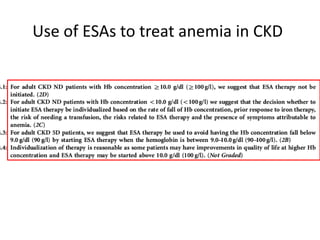
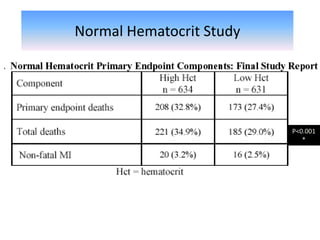
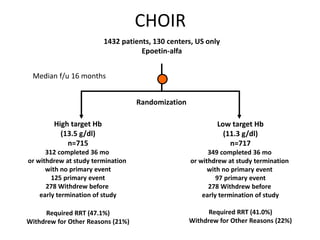
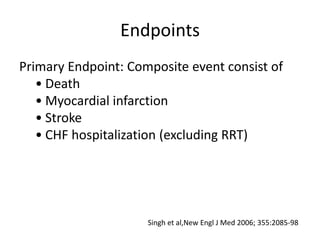
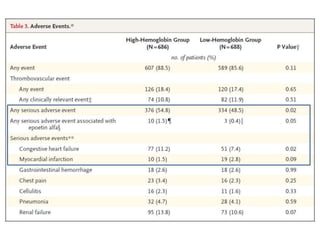
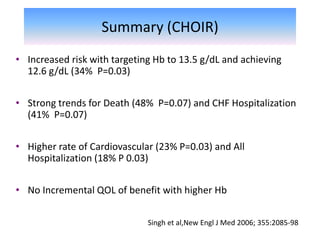
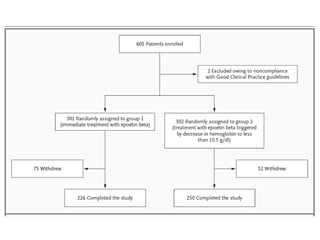
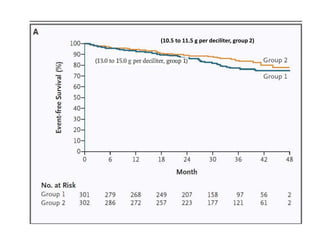
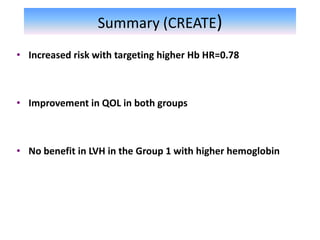
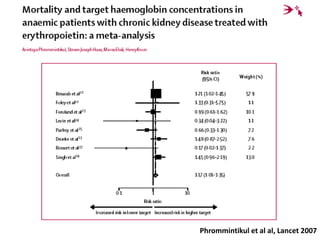




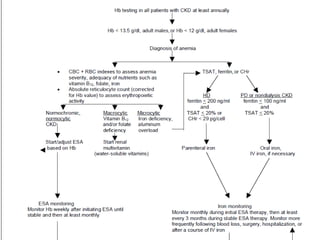

This document discusses anemia management in chronic kidney disease (CKD). It covers the mechanisms of anemia in CKD, including erythropoietin deficiency and iron deficiency. It reviews guidelines for hemoglobin targets and the use of erythropoiesis-stimulating agents (ESAs) to treat anemia. Larger studies on hemoglobin targets in both dialysis and non-dialysis CKD patients, such as the CHOIR and CREATE trials, found higher risks with higher hemoglobin targets and no benefits to quality of life. Iron deficiency is a major cause of ESA treatment failure in CKD patients.






















































![ppt. Anemia in Chronic Kidney Disease (1) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ppt-250726225458-7055b642-thumbnail.jpg?width=640&height=640&fit=bounds)


































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)