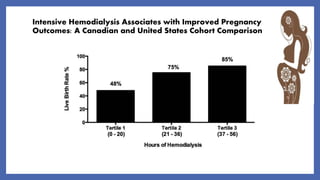
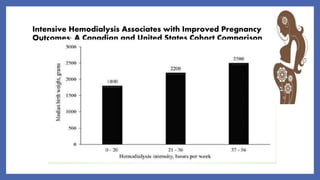
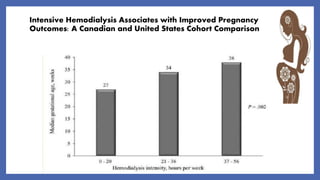
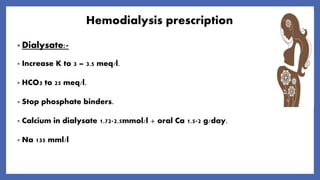
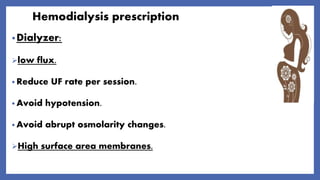
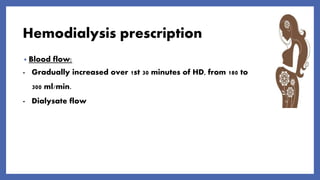
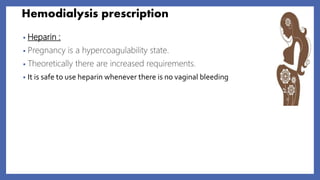
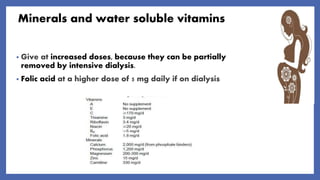
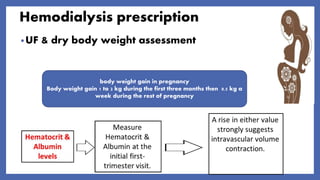
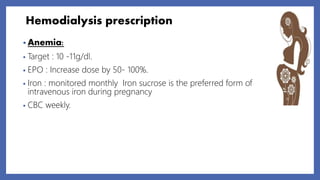
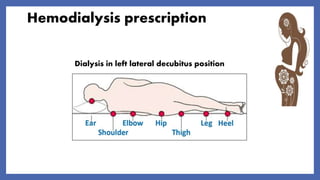
This document discusses the management of pregnant women on hemodialysis. It notes that physiological changes during pregnancy can impact kidney function, but intensive hemodialysis of more than 20 hours per week is recommended to reduce risks. Close monitoring of blood pressure, nutrition, mineral levels, anemia and fetal growth is important. Hemodialysis prescription should be tailored to each patient's needs, with adjustments to dialysate composition and blood flow. Vaginal delivery at 38 weeks is typically recommended unless complications arise. A multidisciplinary team of nephrologists, obstetricians and dietitians helps optimize outcomes for these high-risk pregnancies.