Downloaded 64 times
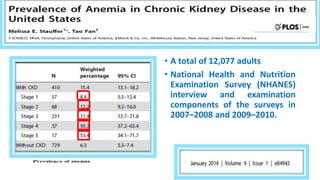
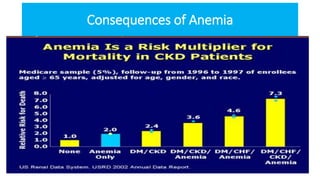

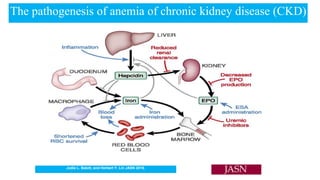
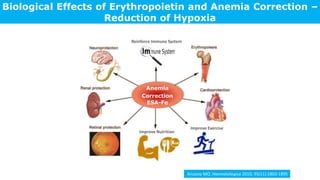
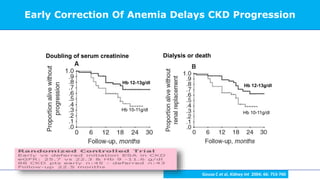




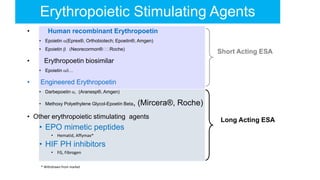



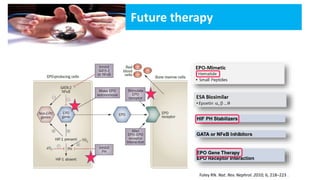
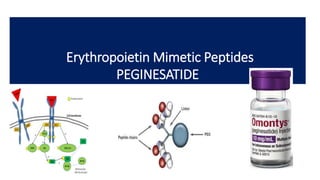


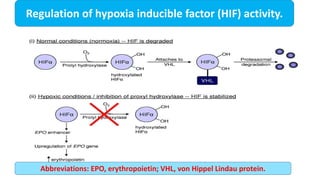
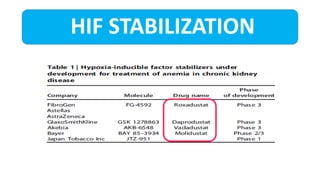
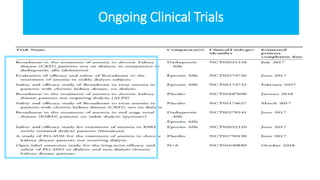

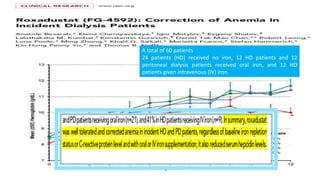
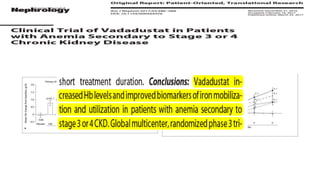

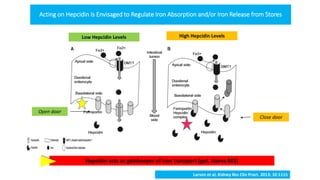
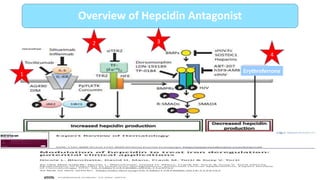







This document summarizes the current state of anemia management in chronic kidney disease patients. It discusses the magnitude of anemia as a problem in CKD patients, outlines the clinical management including first-line treatments like blood saving techniques and second-line treatments like erythropoiesis-stimulating agents and iron supplementation. It also explores future therapy options, noting investigational drugs that aim to stabilize hypoxia-inducible factor or mimic erythropoietin's effects. The document reviews clinical trial data on these new agents and discusses limitations of current erythropoietin-based approaches.







































![Ckd and anemis6295500258461766990[11826]](https://cdn.slidesharecdn.com/ss_thumbnails/ckdandanemis629550025846176699011826-200630165349-thumbnail.jpg?width=640&height=640&fit=bounds)




![ppt. Anemia in Chronic Kidney Disease (1) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ppt-250726225458-7055b642-thumbnail.jpg?width=640&height=640&fit=bounds)










































