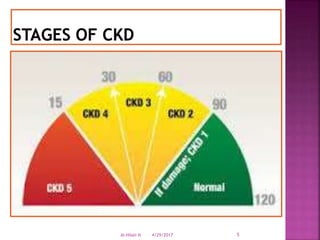
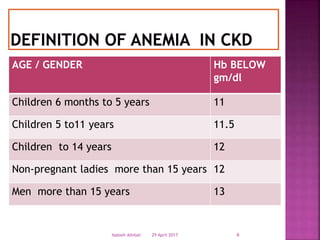
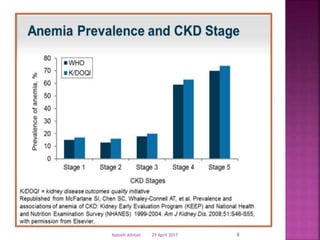
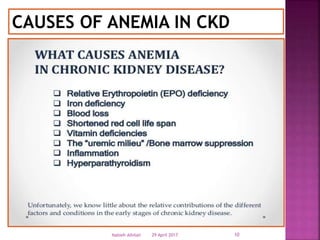
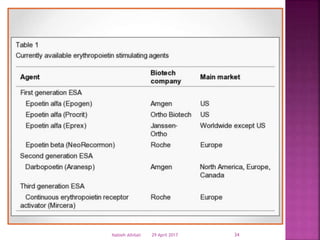
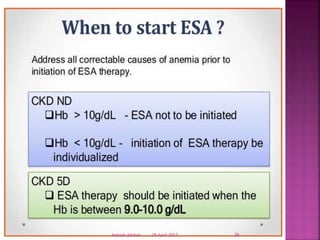
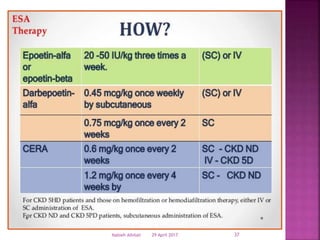
This document discusses the therapeutic landscape for anemia in chronic kidney disease (CKD). It defines CKD and notes that nearly 90% of patients with a glomerular filtration rate below 25-30 mL/min have anemia, often with hemoglobin levels below 10 g/dL. The causes of anemia in CKD are described as well as the effects, which include poorer quality of life, increased risk of cardiovascular disease and mortality, and accelerated progression of kidney disease. Therapeutic options discussed include iron therapy to maintain sufficient iron stores, erythropoiesis-stimulating agents (ESAs) to treat anemia, blood transfusion in some cases, and investigational therapies. The risks of ESAs at higher

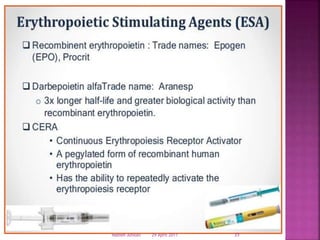
![ They are used in treating anemia resulting
from chronic kidney disease,
chemotherapy induced anemia in patients
with cancer,
inflammatory bowel disease (Crohnes
disease and ulcerative colitis)[20] and
myelodysplasia from the treatment
of cancer (chemotherapy and radiation).
29 April 2017 33Nabieh Alhilali](https://image.slidesharecdn.com/esa2-170429125704/85/Esa-2-33-320.jpg)




































![Ckd and anemis6295500258461766990[11826]](https://cdn.slidesharecdn.com/ss_thumbnails/ckdandanemis629550025846176699011826-200630165349-thumbnail.jpg?width=640&height=640&fit=bounds)
![ppt. Anemia in Chronic Kidney Disease (1) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ppt-250726225458-7055b642-thumbnail.jpg?width=640&height=640&fit=bounds)






























