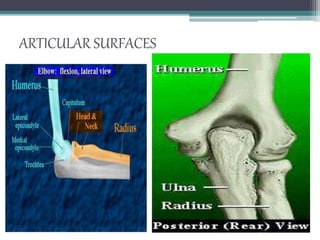
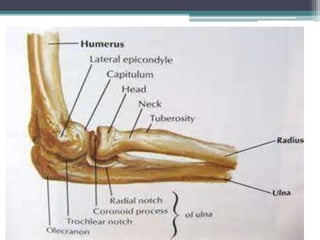
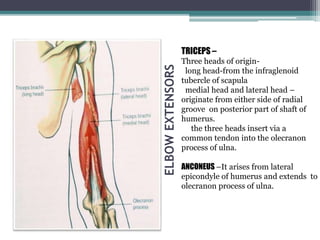
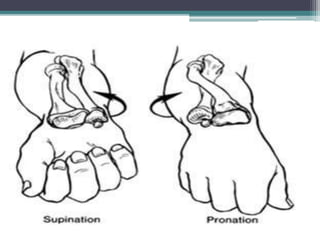
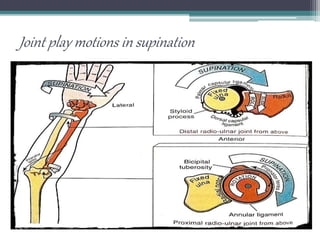
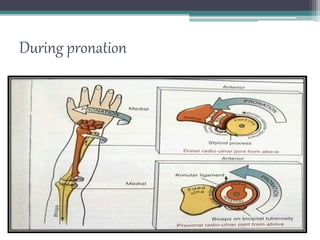
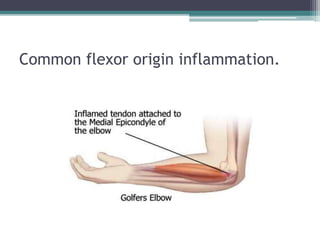
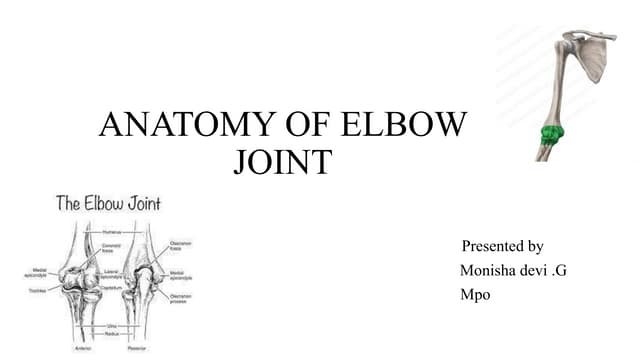
The elbow complex is composed of three joints that allow hinge and rotational movements. It includes the humeroulnar joint formed by the trochlea of the humerus articulating with the ulna, the humeroradial joint formed by the capitulum articulating with the radius, and the proximal and distal radioulnar joints. Various ligaments like the medial and lateral collateral ligaments stabilize the elbow joints. Muscles like the triceps, brachialis, and biceps are involved in elbow flexion while the triceps and anconeus extend the elbow. The pronators and supinators control forearm rotation. Injuries like tennis elbow or pulled elbow in