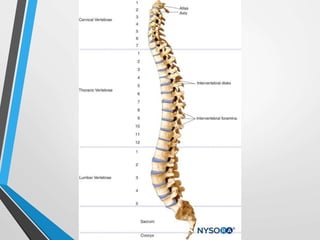
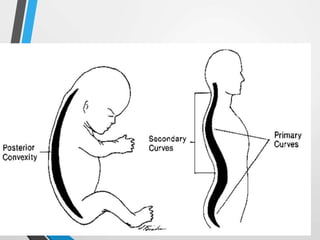
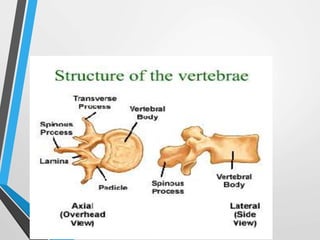
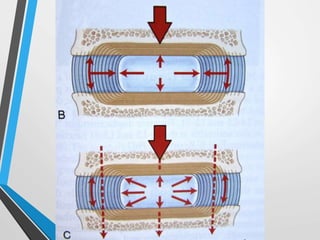
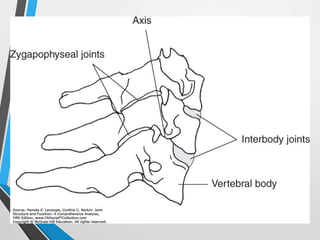
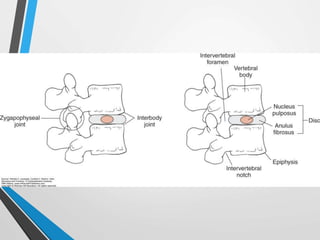
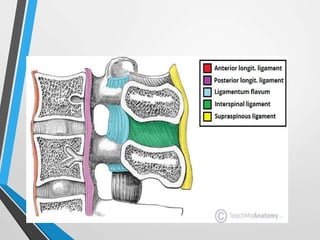
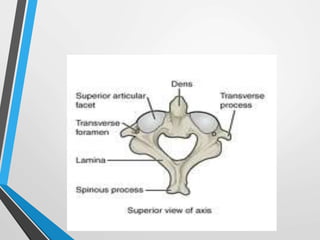
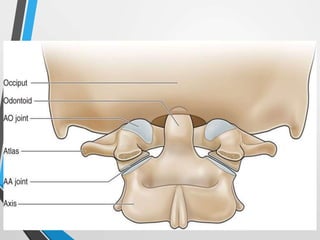
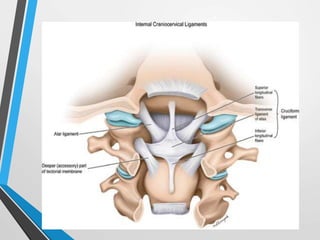
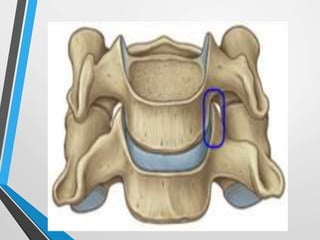
The document summarizes the biomechanics of the vertebral column. It describes the typical structure and regions of the vertebral column. It then discusses the typical vertebrae structure, intervertebral discs, articulations, ligaments, curves of the spine, and kinetics and kinematics including forces like compression, bending, torsion and shear. It also provides details on the specific structure and features of the cervical spine regions.