Downloaded 725 times










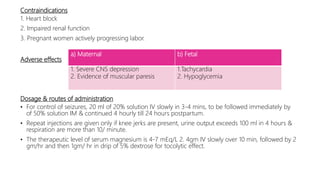
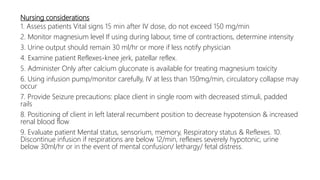
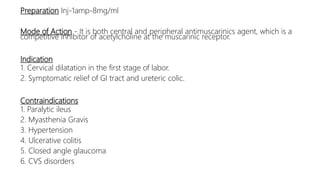






The document discusses drugs used during pregnancy, labor, and the postpartum period. It provides information on folic acid, iron, calcium, antihypertensive drugs, diuretics, tocolytic agents, oxytocics, analgesics, and anticoagulants. For each drug, it describes preparations, mode of action, indications, contraindications, adverse effects, dosage, and important nursing considerations. The document is intended to give nurses thorough knowledge of medications commonly administered during obstetric care.