Downloaded 1,745 times

![EXPECTANT MANGEMENT
Controlled cord traction [ modified
Brandt-Andrews method]:](https://image.slidesharecdn.com/thirdstageoflabour-140413065917-phpapp01/75/Third-stage-of-labour-13-2048.jpg)
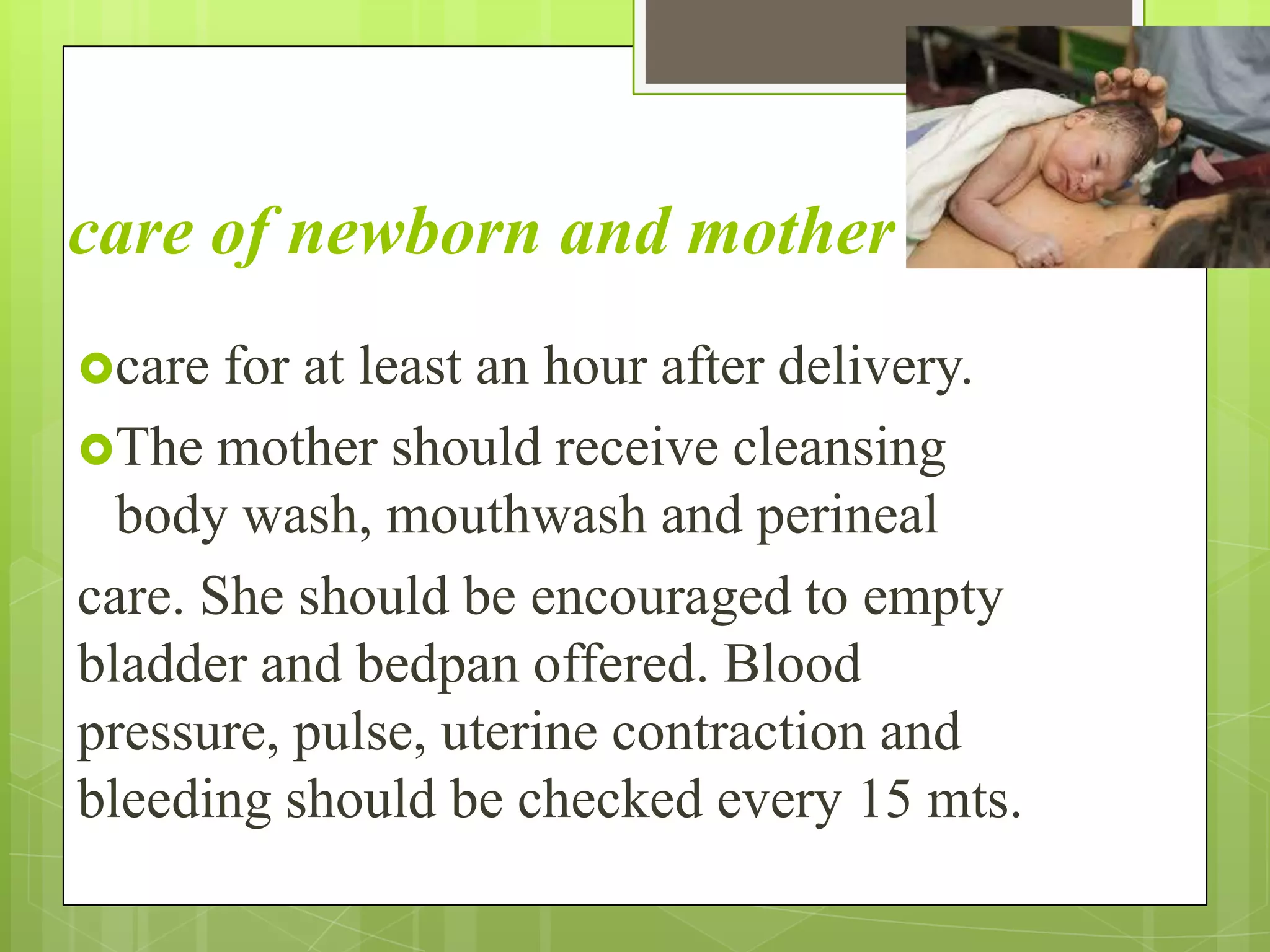
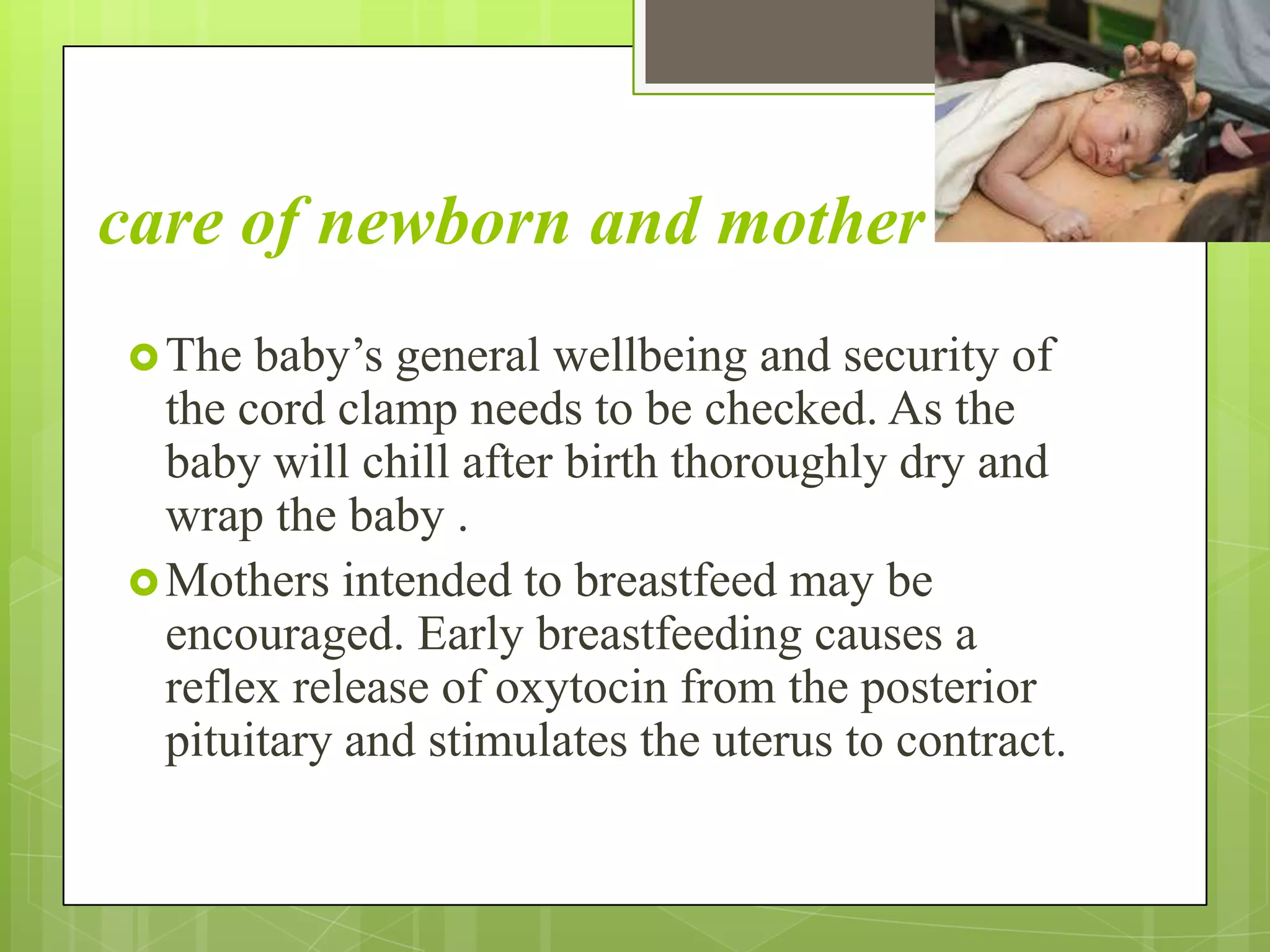

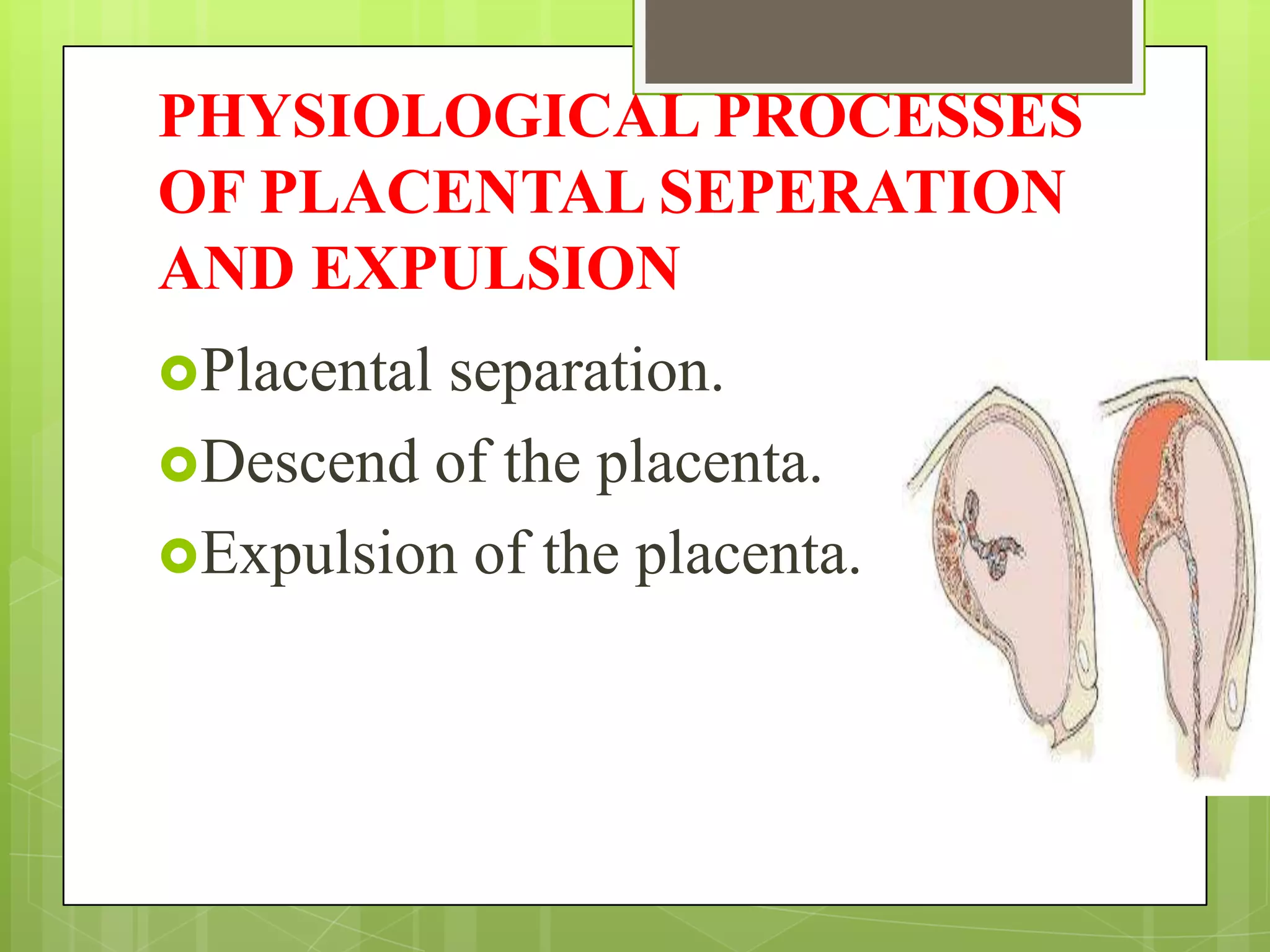
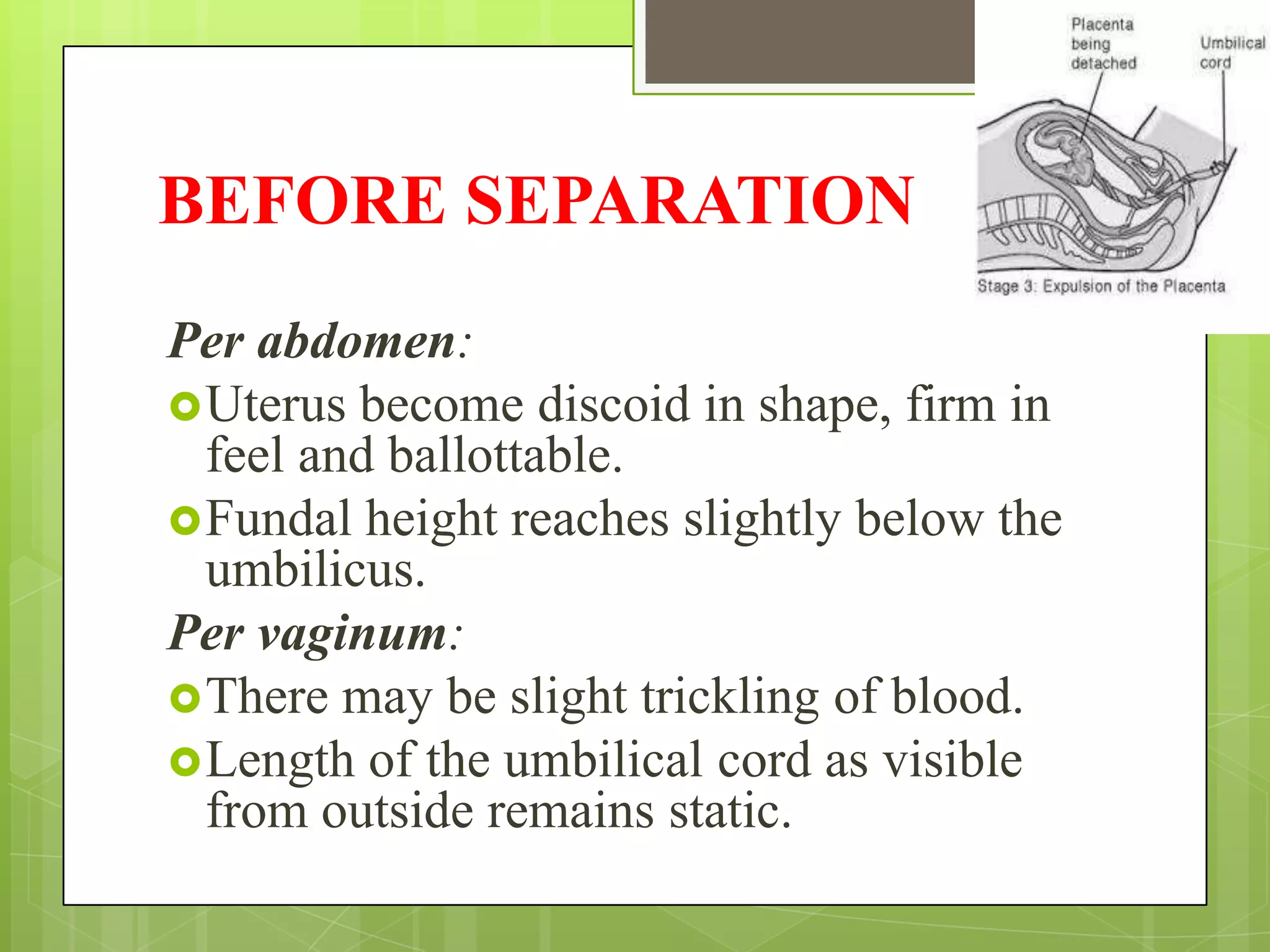
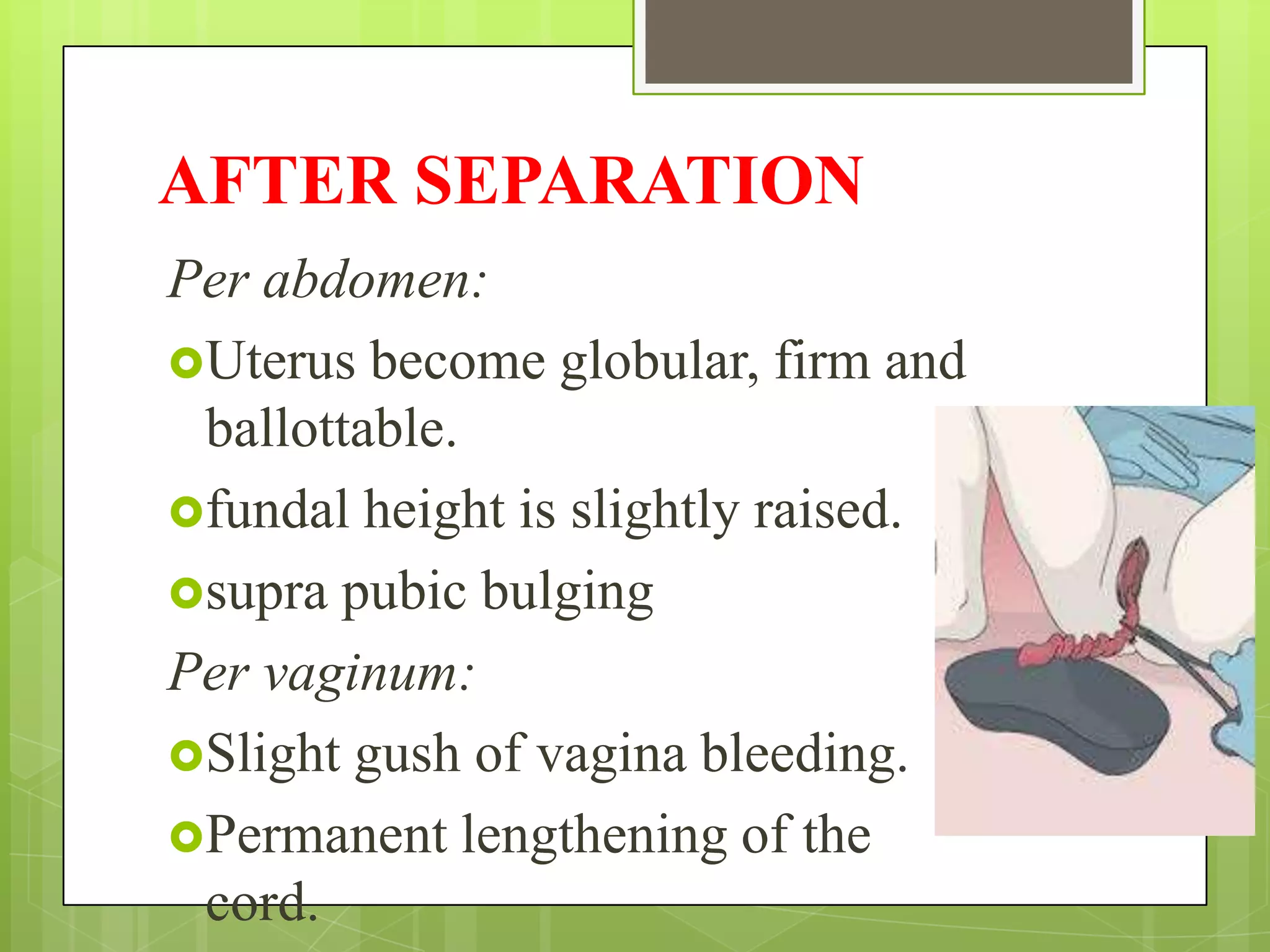
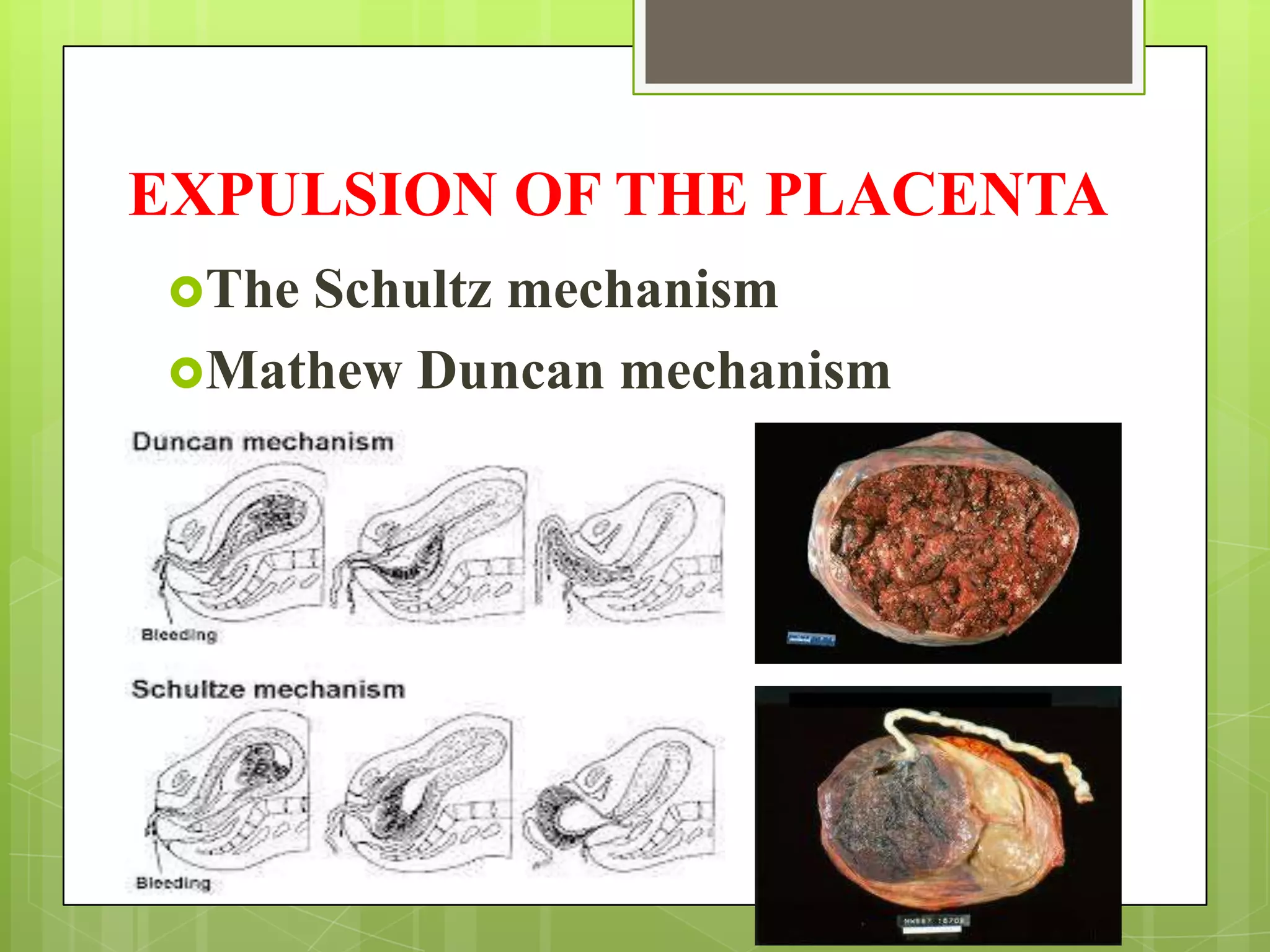
The third stage of labor involves the separation and expulsion of the placenta after childbirth. The placenta separates from the uterine wall due to uterine contraction. The uterus then contracts further to aid the descent and expulsion of the placenta through the birth canal. Midwives monitor for signs of separation and use techniques like controlled cord traction or fundal pressure to deliver the placenta if needed. Oxytocic drugs may also be used to aid delivery or prevent hemorrhage. Care of both mother and newborn continues for at least an hour after completion of the third stage to ensure uterine contraction and monitor for complications.







































































































