Downloaded 96 times































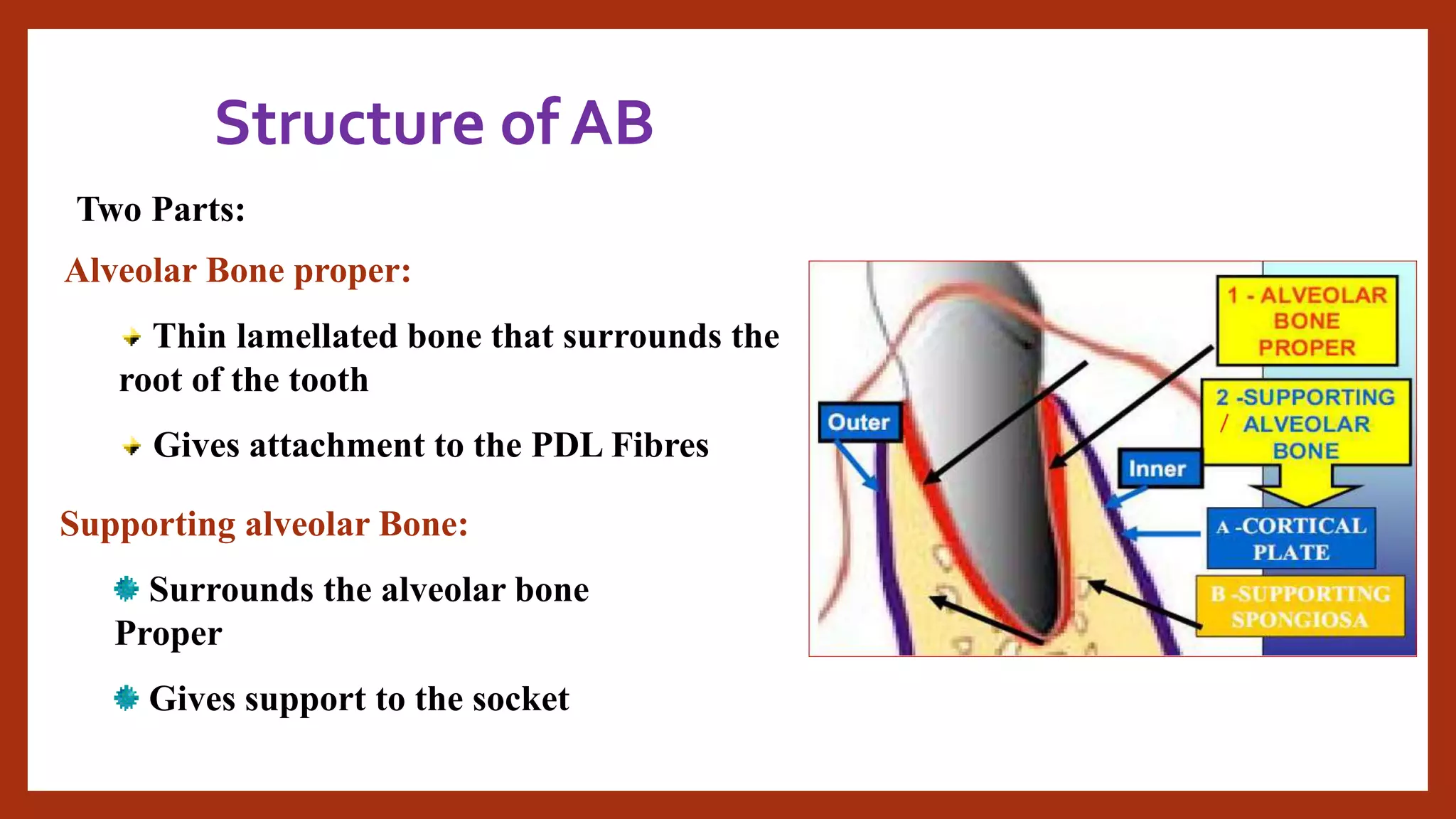





























The document provides an overview of alveolar bone, including its development, structure, blood and nerve supply, functions, and clinical considerations. Alveolar bone develops with the formation and eruption of teeth and supports the teeth by forming the bony sockets within the maxilla and mandible. It has two parts - the alveolar bone proper that directly surrounds the tooth root and the supporting alveolar bone that provides structural support. Age-related changes such as loss of bone with tooth loss are discussed. Therapeutic options for treating alveolar bone defects through grafting and regeneration techniques are also summarized.























































































