Downloaded 50 times












































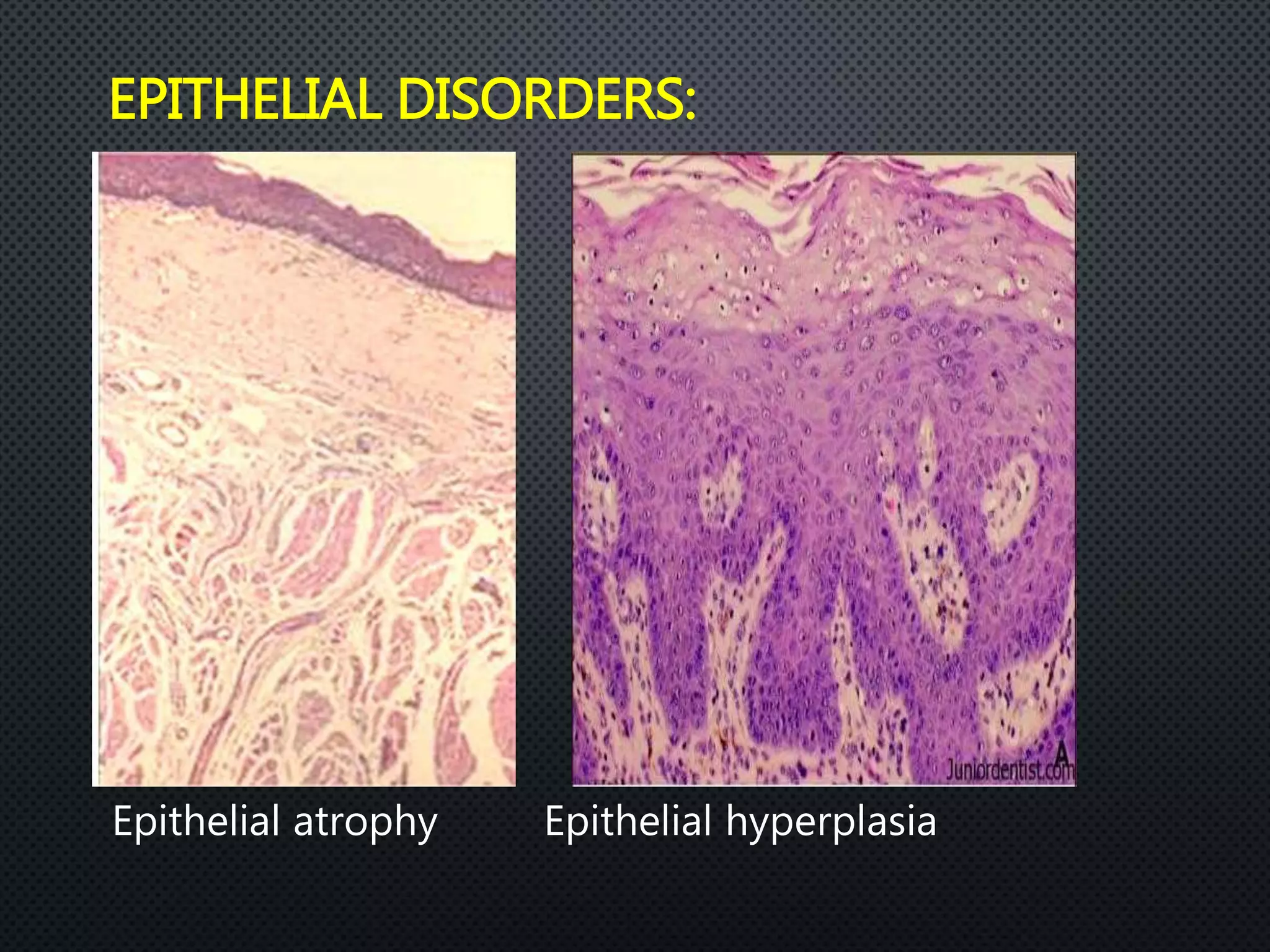














The oral epithelium acts as a protective barrier for the oral mucosa. It is composed of keratinocytes that undergo proliferation and maturation as they move from the basal layer to the surface. Keratinocytes express different cytokeratins as they mature and differentiate. The oral epithelium can be keratinized or non-keratinized depending on its location. A basement membrane anchors the epithelium. Various cellular disorders can affect the oral epithelium. Non-keratinocytes including melanocytes, Langerhans cells, and lymphocytes are also present in small numbers.














































































