Downloaded 305 times




































![• Functional ligaments- Serve as major anatomical
component for the joint.
a] Collateral/Discal ligament
b] Capsular ligament
c] Temporomandibular ligament
• Accessory ligaments-Serve as passive restraints to
mandibular motion.
a] Sphenomandibular ligament.
b] Stylomandibular ligament.](https://image.slidesharecdn.com/3tmj-161031032449/85/TMJ-39-320.jpg)





























































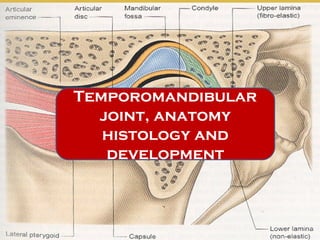
The document discusses the development, anatomy, and histology of the temporomandibular joint (TMJ). It identifies three phases of TMJ development: the blastematic stage from weeks 7-8, the cavitation stage from weeks 9-11, and the maturation stage after week 12. The TMJ is a complex joint that involves the temporal bone, mandibular condyle, articular disc, and various ligaments, and its development and structure are important for understanding clinical management of the joint.























































































