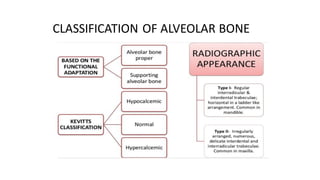
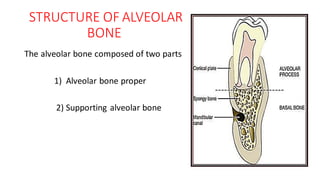
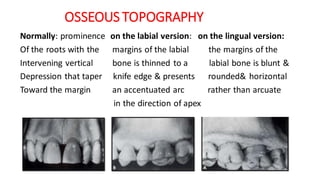
The document provides information about alveolar bone, including its development, functions, composition, classification, gross morphology, histology, bone formation, bone resorption, and bone remodeling. It defines alveolar bone as the portion of maxilla and mandible that forms and supports the tooth socket. It develops from the dental follicle during tooth eruption. The size and shape of alveolar bone is dependent on the teeth. It has important functions like housing tooth roots and providing attachment for the periodontal ligament and muscles.












































![• The leading edge of resorption –
Cutting cone
• Released cytokines [ BMP & IGF]
stimulate stem cells to
differentiate into osteoblasts.
• osteoblasts secrete osteoid -
Filling cone](https://image.slidesharecdn.com/alveolarbonenew-200624043058/85/Alveolarbone-55-320.jpg)

































































![ALVEOLAR BONE IN HEALTH AND DISEASE [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/alveolarboneinhealthanddiseaseautosaved-231125051936-9d7ab2b3-thumbnail.jpg?width=640&height=640&fit=bounds)




















