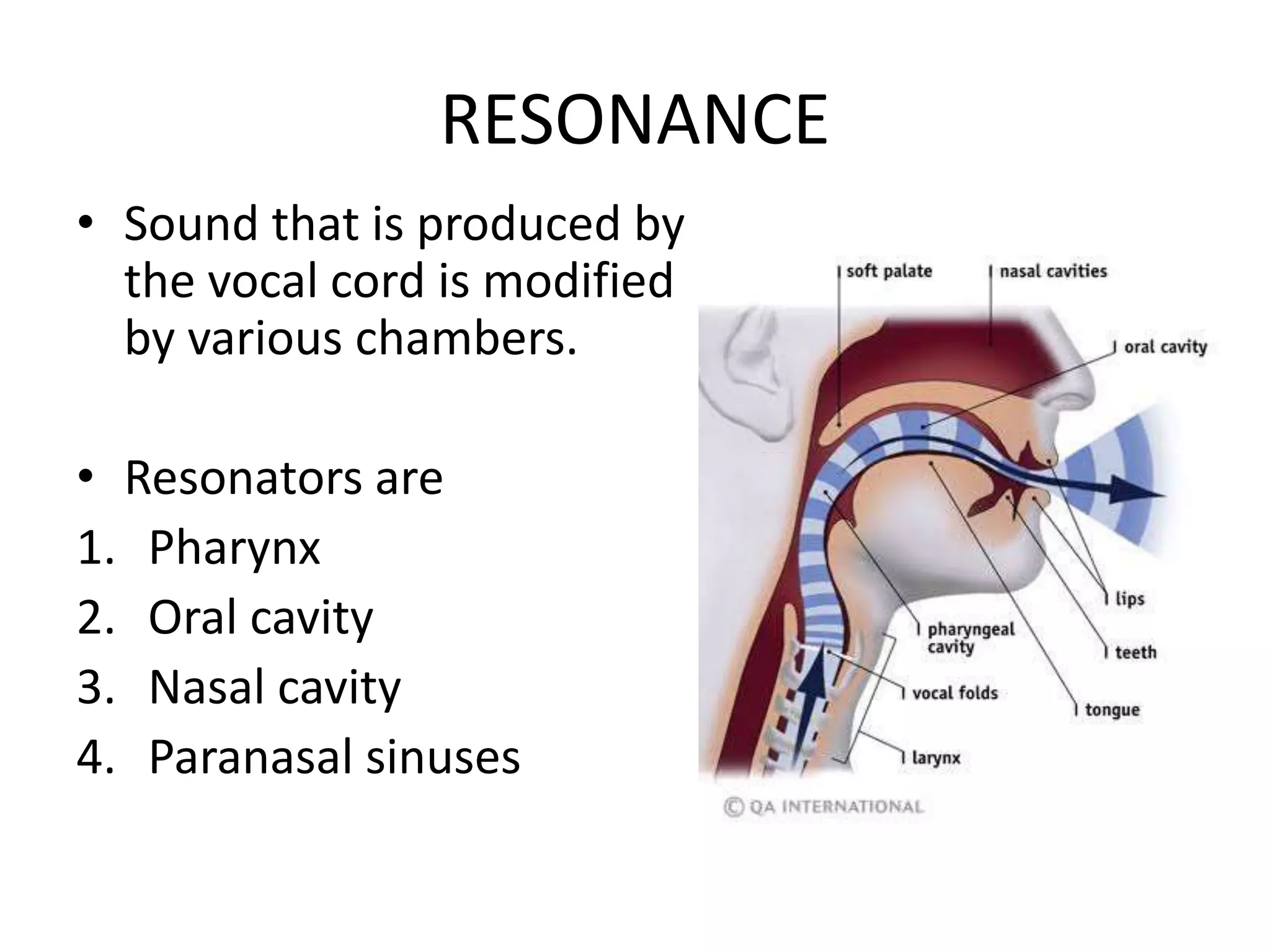
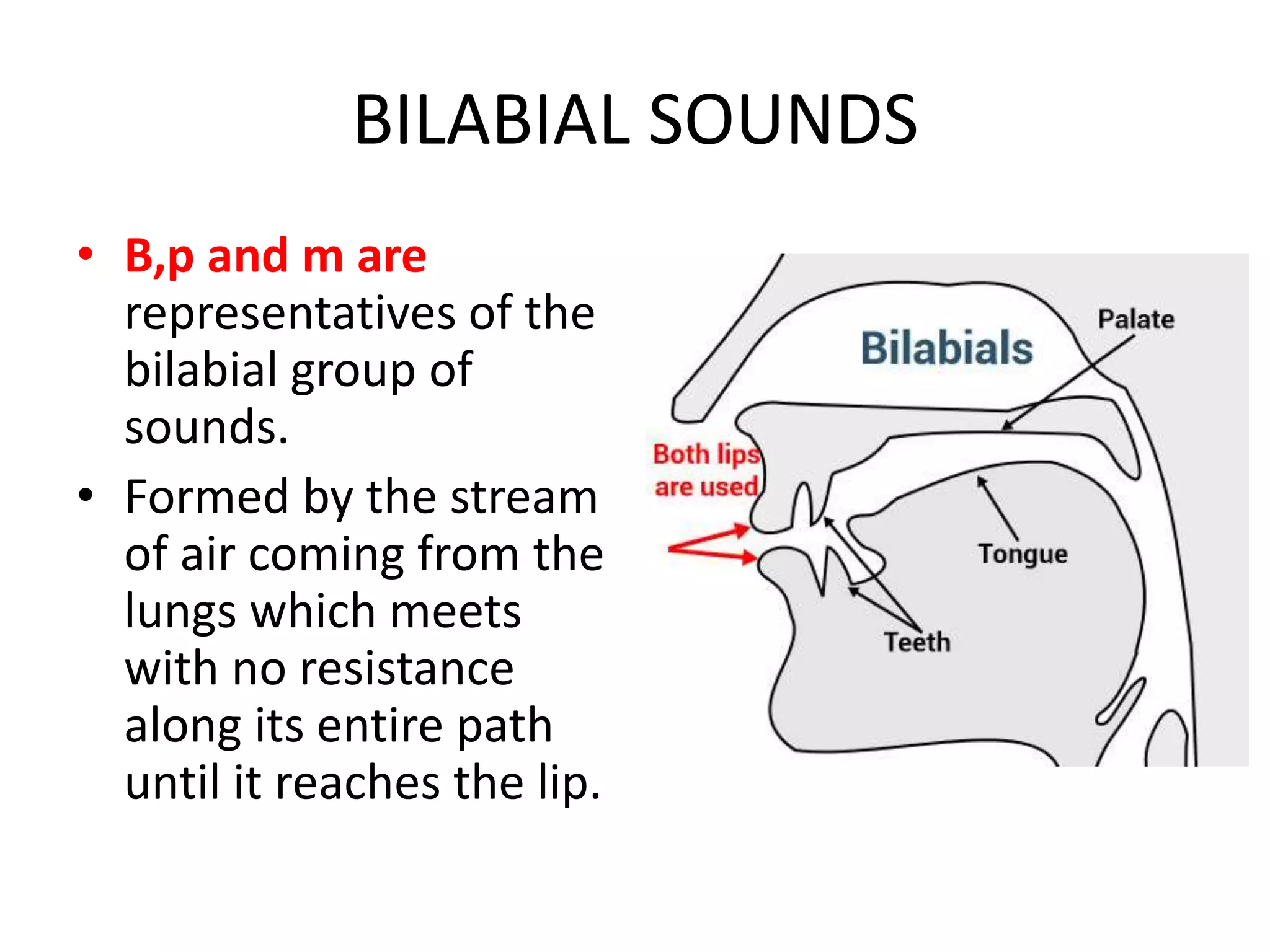
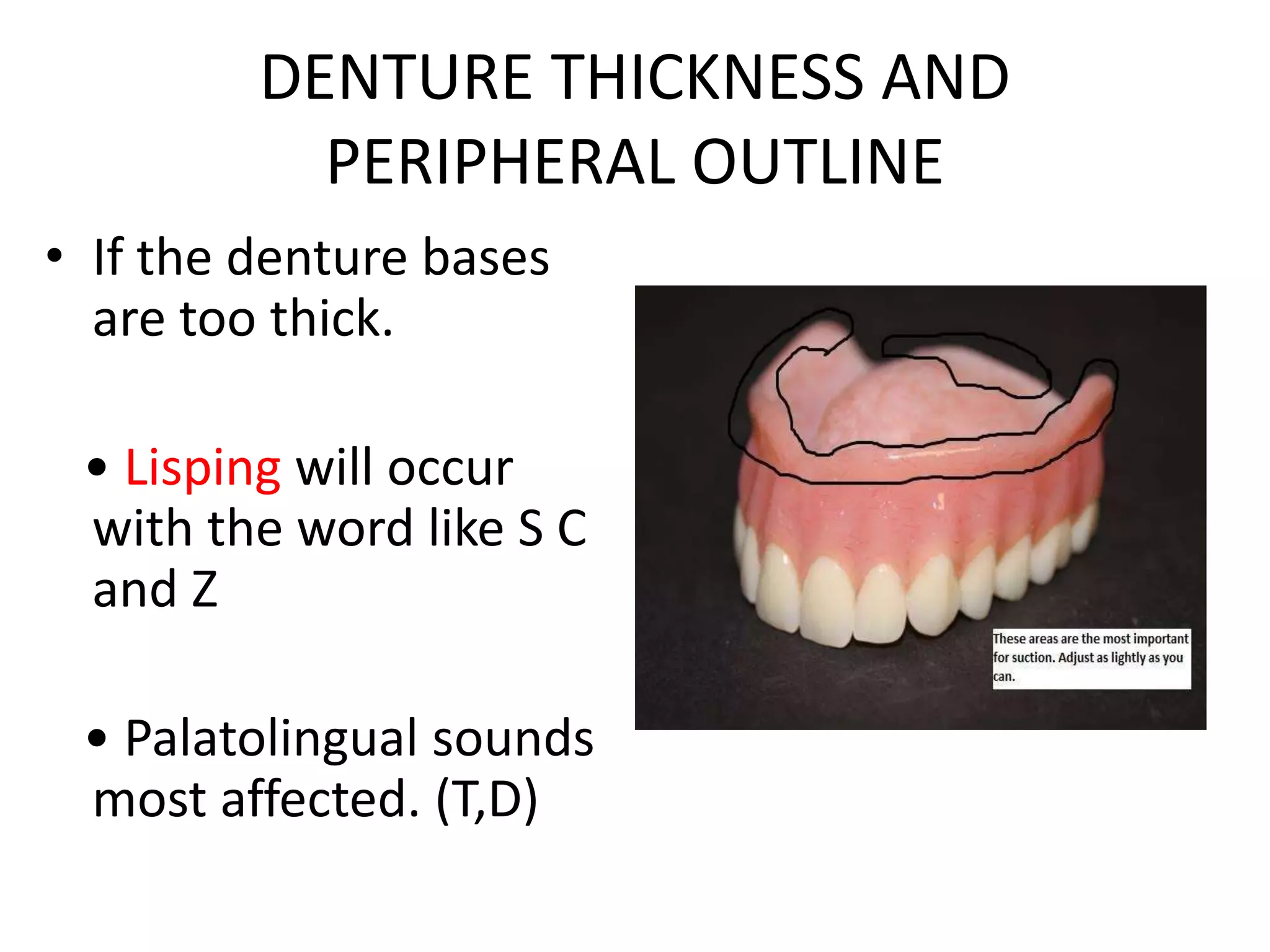
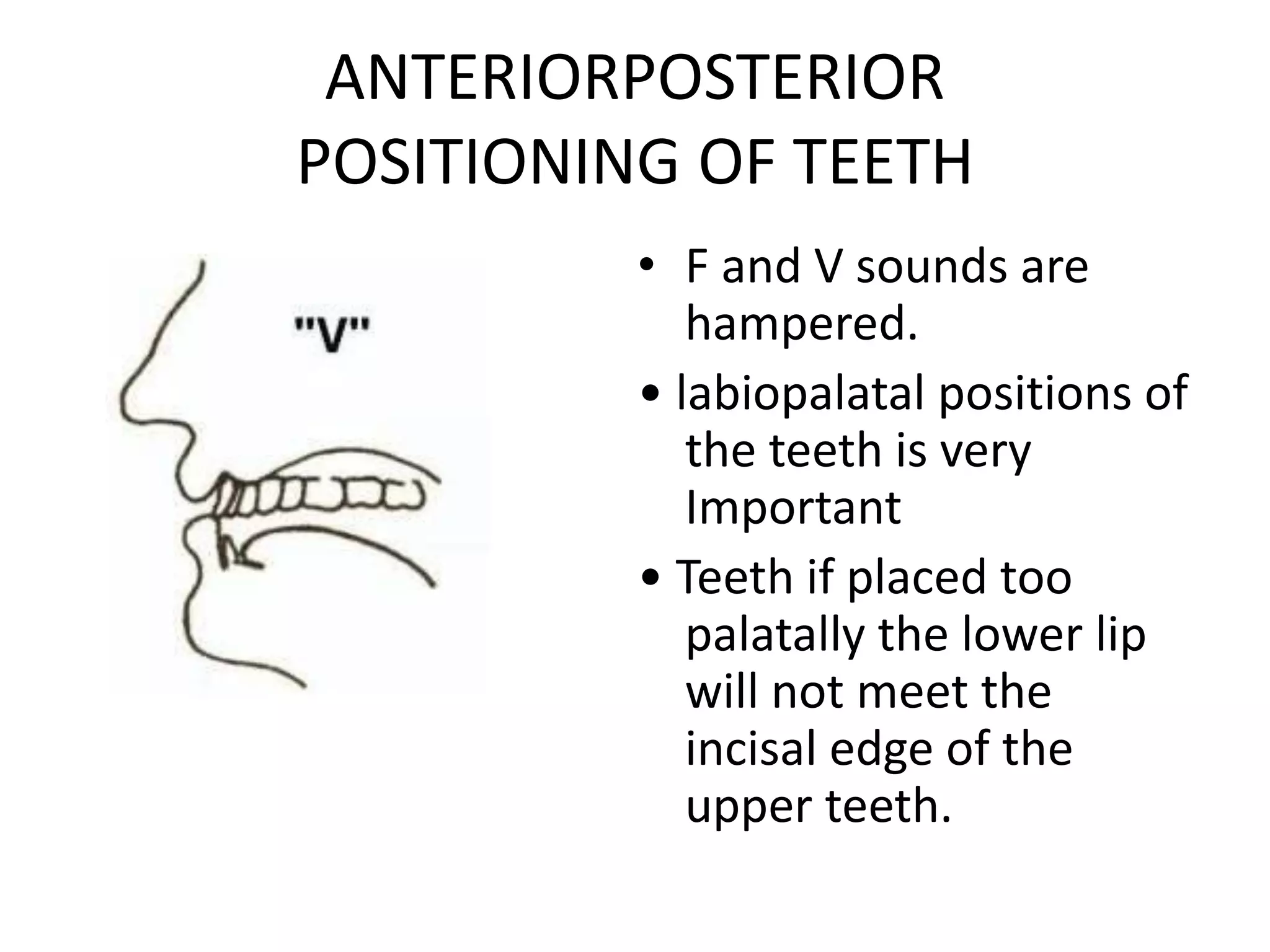
The document discusses the significance of phonetics in the design and adaptation of complete dentures and its implications for speech. It outlines various aspects such as the mechanisms of speech production, the classification of speech sounds, and the clinical significance of proper denture fit on articulatory function. Various tests and their importance in evaluating speech post-denture insertion are also detailed, emphasizing the necessity for adjustments in denture design to support clear articulation.