Downloaded 33 times
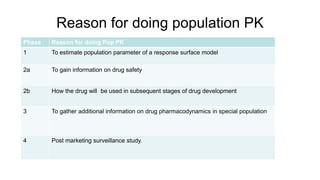



The document outlines the objectives and principles of population pharmacokinetics, emphasizing its significance in understanding variability in drug concentrations among different patient populations. It discusses the development of population pharmacokinetics, Bayesian theory, and adaptive methods used to enhance dosage strategies and pharmacokinetic parameter estimations. Furthermore, it highlights the challenges and advantages of population pharmacokinetics in drug development and clinical applications.








































![[DSC Europe 23][DigiHealth] Katarina Vucicevic - Navigating theKinetics of Dr...](https://cdn.slidesharecdn.com/ss_thumbnails/w0gtqyyysv2u5fguv9wa-katarina-vucicevic-navigating-the-kinetics-of-drugs-through-data-insights-clean-231130131010-27415132-thumbnail.jpg?width=640&height=640&fit=bounds)













































