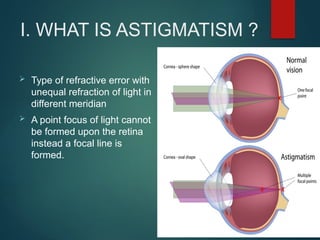
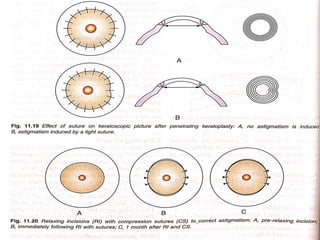
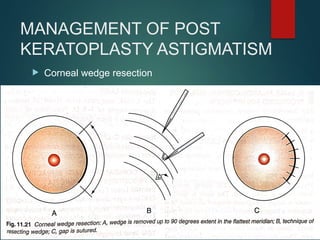
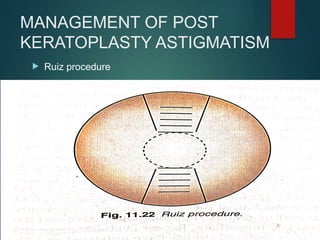
This document covers astigmatism, a type of refractive error characterized by unequal light refraction in different meridians, leading to visual distortion. It details the types, causes, symptoms, diagnostics, and treatment options for astigmatism, including optical and surgical methods. Various investigations and their applications, along with the management strategies for post-keratoplasty astigmatism, are also discussed.