Downloaded 44 times


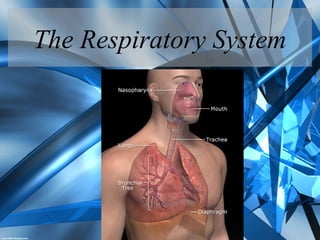
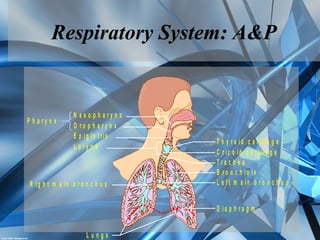
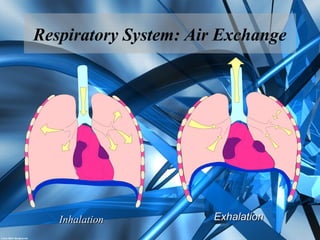
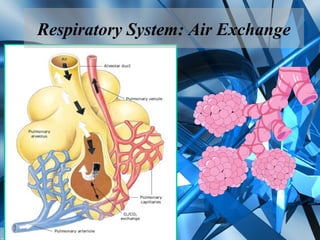
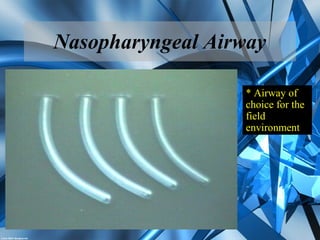

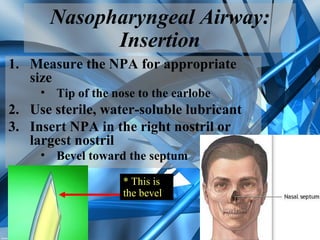
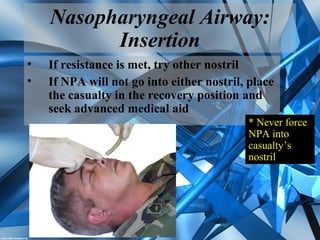
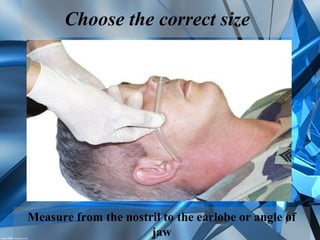
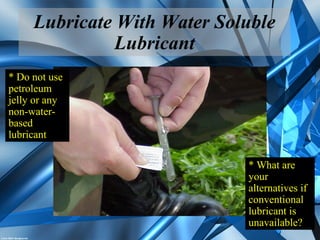

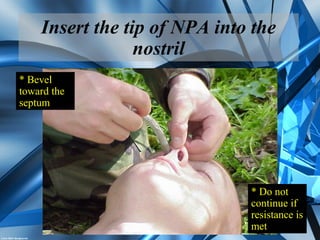
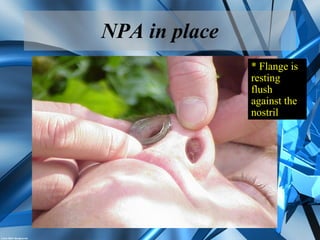
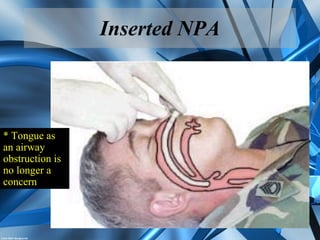
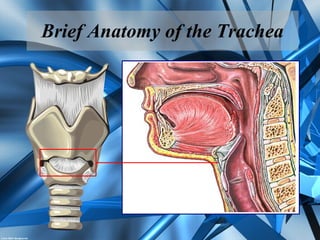
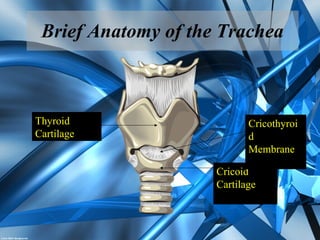
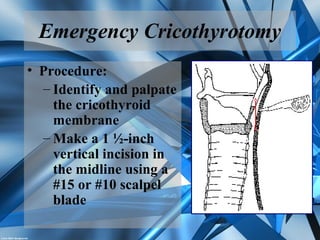
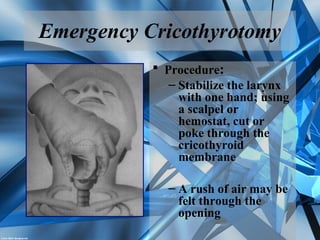
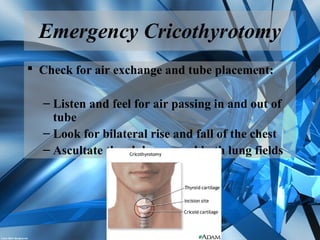



This document provides instruction on airway management for soldiers. It covers (1) the anatomy and physiology of the respiratory system, (2) how to identify adequate and inadequate breathing, (3) how to evaluate an unconscious casualty, (4) how to insert a nasopharyngeal airway, and (5) how to perform an emergency cricothyrotomy procedure. The goal is to teach soldiers critical skills for maintaining a casualty's airway to prevent death from respiratory failure.