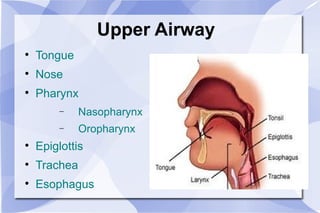
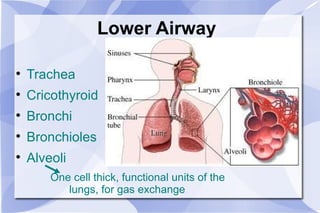
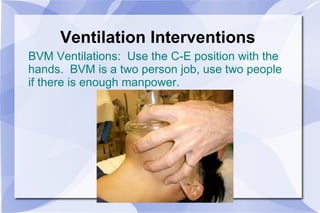
The document provides an overview of airway and breathing topics for continuing education. It covers anatomy and physiology of the upper and lower airways, oxygenation and ventilation processes, clinical assessment techniques, and interventions to ensure proper oxygenation and ventilation including positioning, airway adjuncts, bag-valve-mask ventilation, and advanced airway placement like laryngeal mask airways. Key skills like auscultation, suctioning, and assisting ventilation are also reviewed.