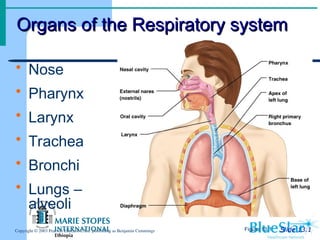
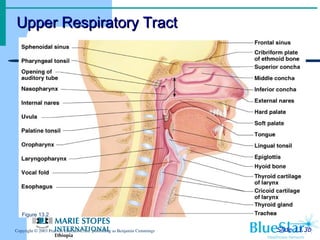
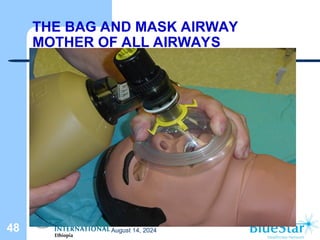
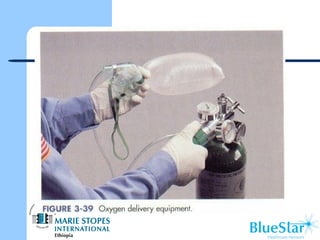
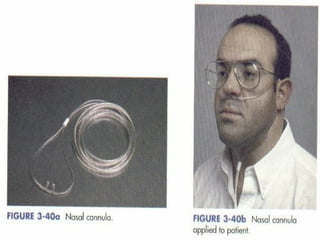
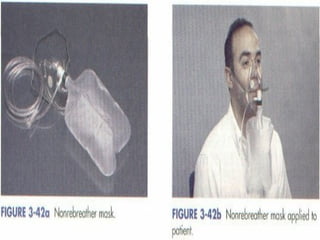
The document discusses the functions and anatomy of the respiratory system, emphasizing its role in gas exchange and the importance of maintaining an open airway. It details various causes of airway obstruction, methods of managing obstructions, and techniques for airway maintenance, including the use of oropharyngeal and nasopharyngeal airways. Additionally, it covers oxygen administration techniques and the use of bag-valve mask ventilation in emergencies.