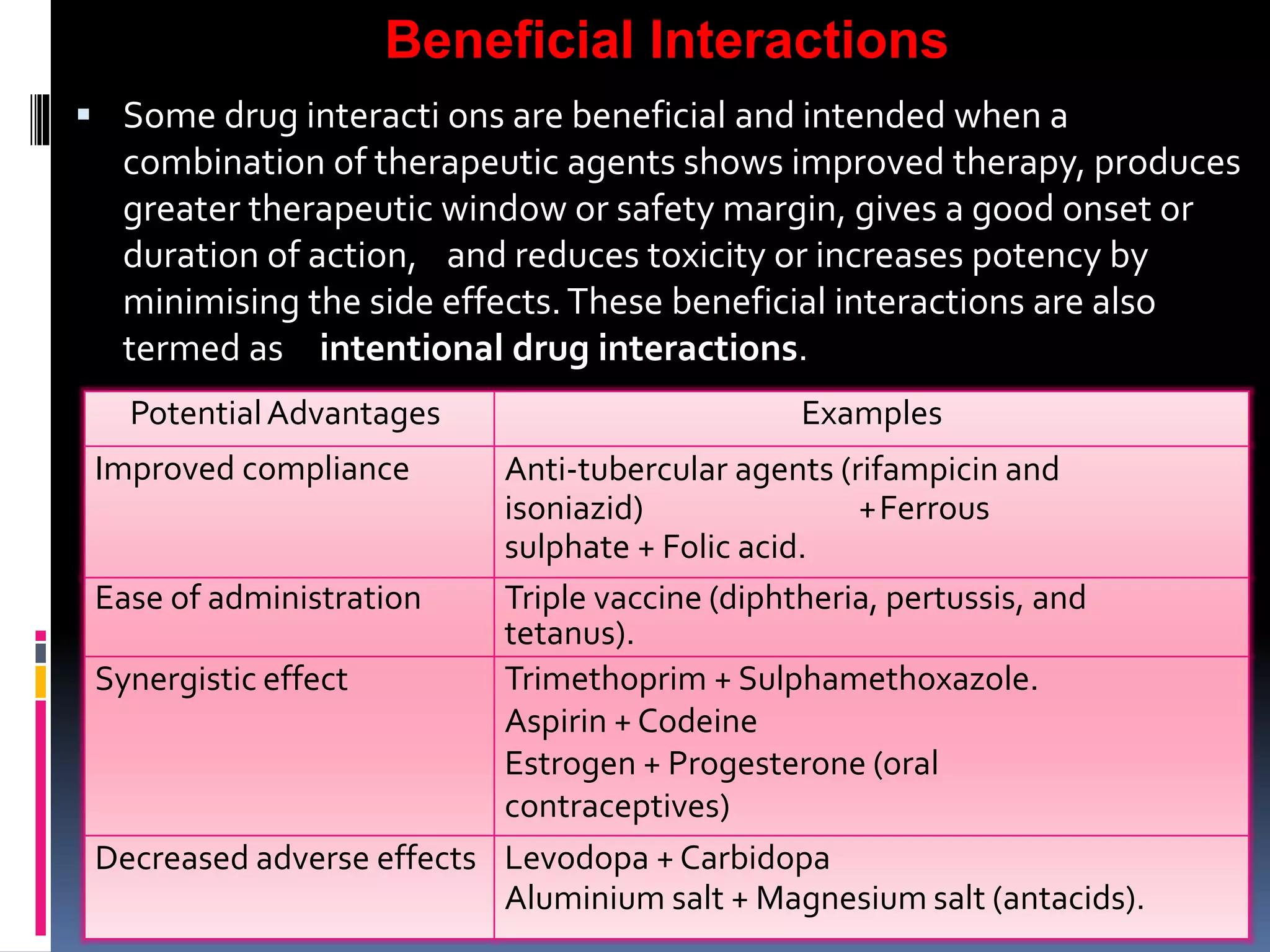
This document discusses drug interactions, including types of interactions and examples. It begins by defining a drug interaction as when one substance affects the activity of another drug. Interactions can occur between drugs, drugs and foods, or drugs and herbs. Some interactions are beneficial when they improve therapy, while adverse interactions counteract therapeutic effects. Examples of interacting drug classes include analgesics, diuretics, cardiovascular drugs, gastrointestinal drugs, vitamins, and hypoglycemic drugs. Methods for detecting interactions include pharmacovigilance using spontaneous case reports and record linkage studies, as well as epidemiological methods like case-control and cohort studies. The document emphasizes the importance of reporting adverse drug reactions.