Downloaded 321 times










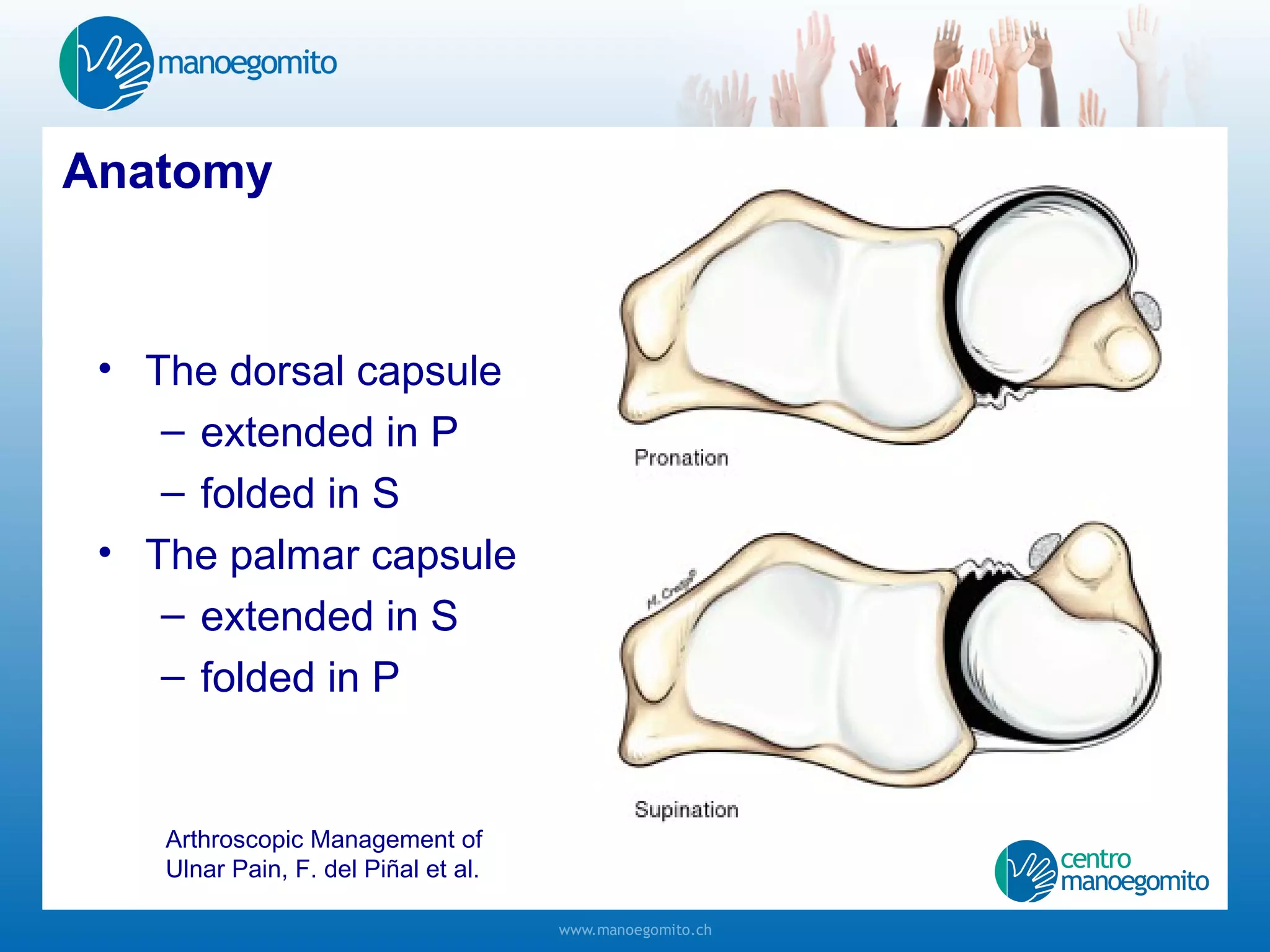

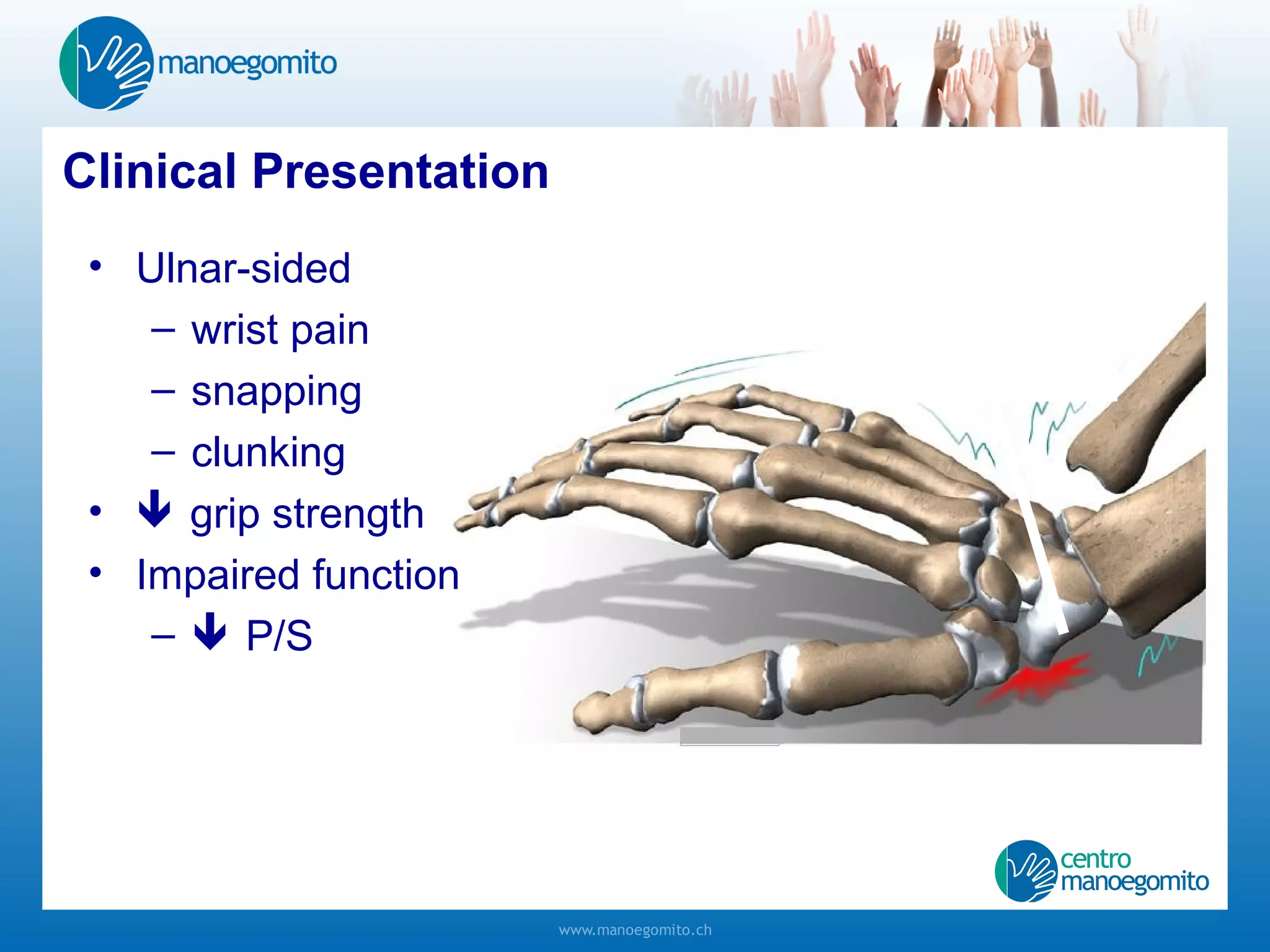

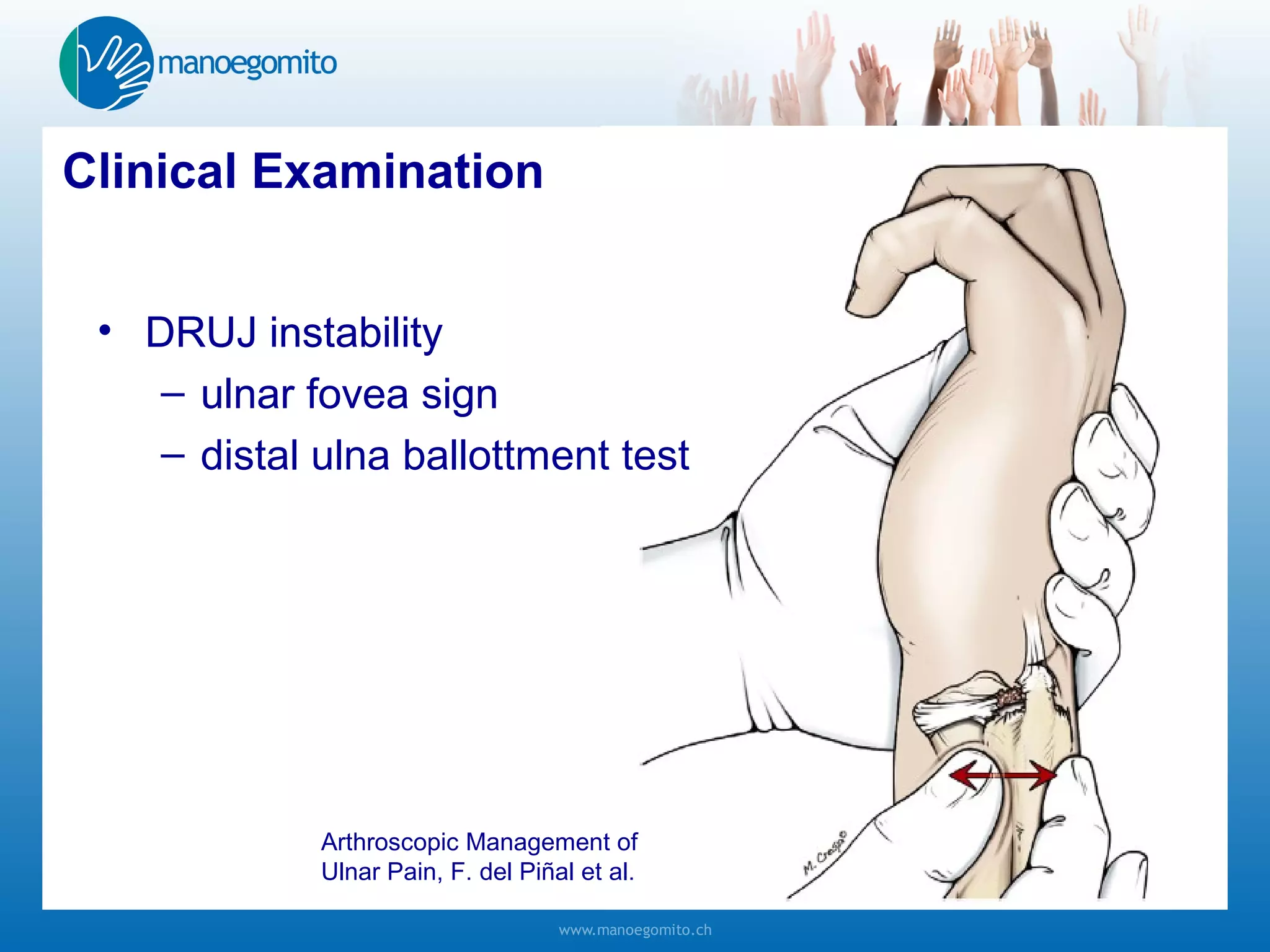









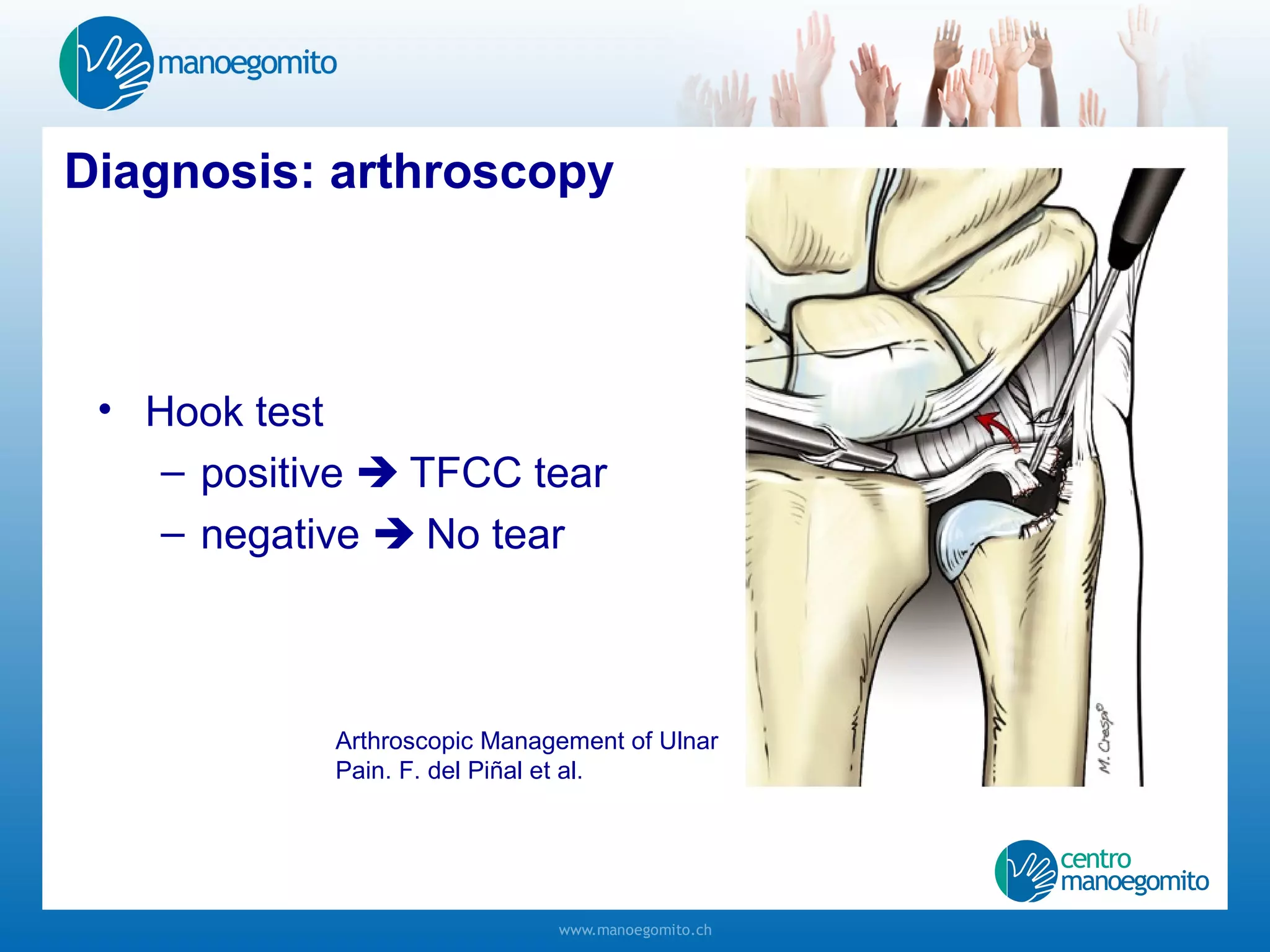








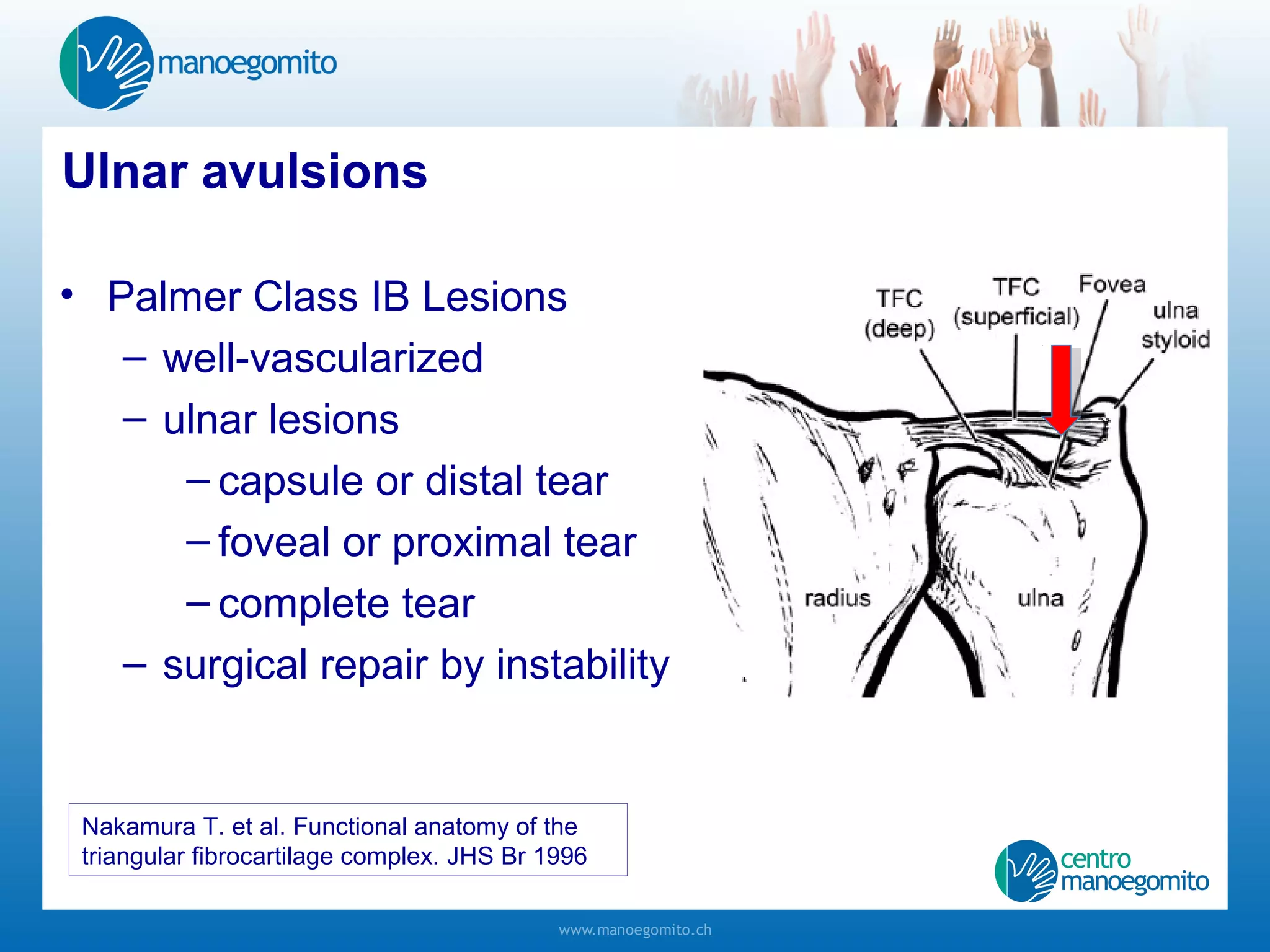
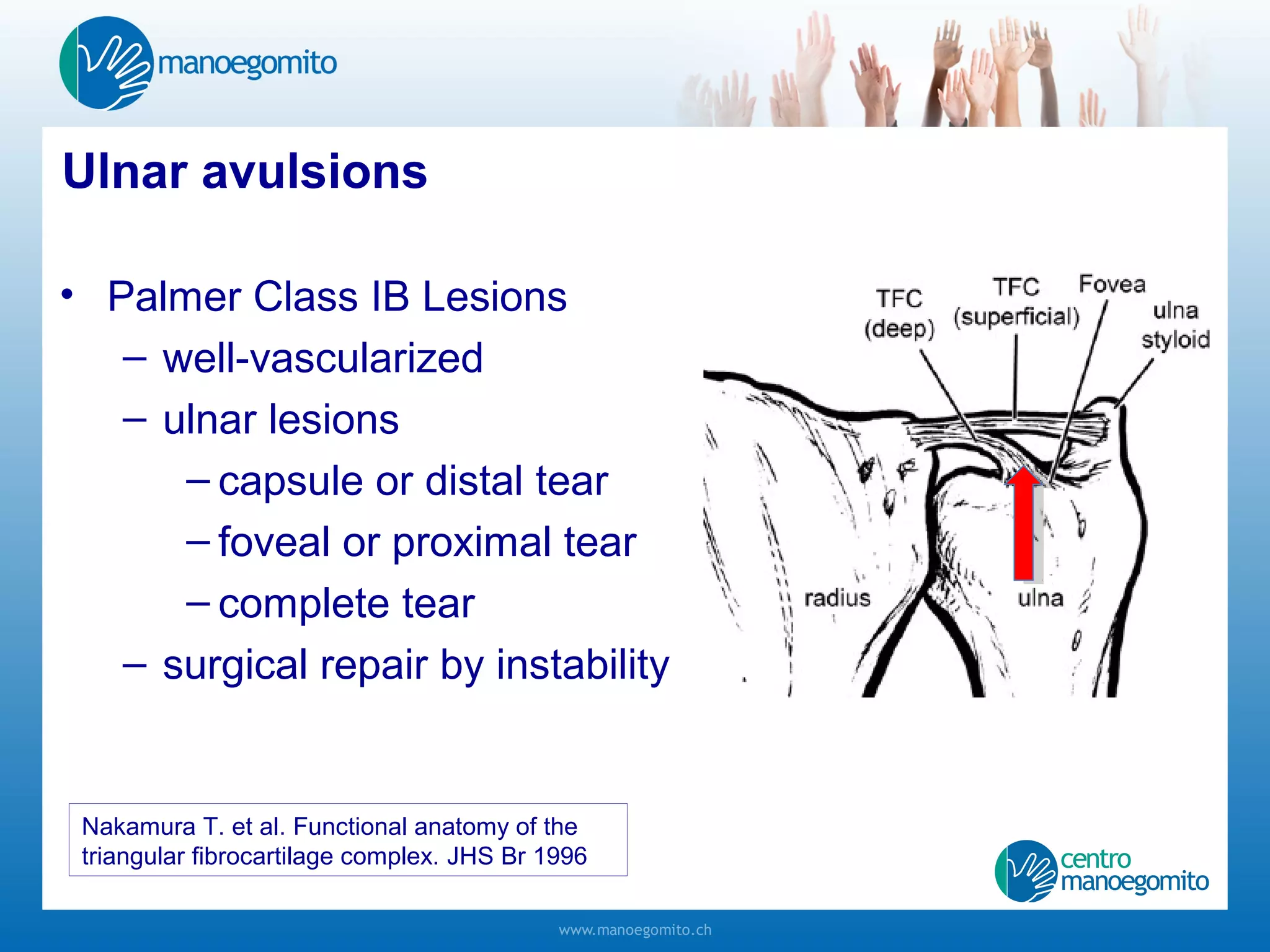


















1) The triangular fibrocartilage complex (TFC) provides stability to the distal radioulnar joint (DRUJ) and allows for forearm pronation and supination. Injuries to the TFC can cause ulnar-sided wrist pain and DRUJ instability. 2) Clinical examination of TFC injuries may reveal DRUJ instability on tests like the ulnar fovea sign and distal ulna ballottment test. MRI or arthroscopy can help diagnose the specific type of TFC tear. 3) Surgical treatment depends on the type and location of the TFC tear. Debridement is used for central perforations while suture repair or foveal









































































































